

Knee pain is a common presentation for clients of any range of age and gender.
Knee pain indeed is a vast topic.
So in this post, we are going to go through how to identify the reason why we can experience knee pain.
For doing so we are going to look at some special testing, that we use for the knee joints.
Next, in a further post, we may analyse individual conditions.
What about the Knee Joint?
The knee is the strongest joint in the body.
It takes a lot of pressure from the upper body and still has to handle the shock coming from the lower leg session, shock as walking, running and jumping.
Indeed, whenever we do one of these actions, the knee plays a big role.
Knee Anatomy
Bond:
- Above: Femur
- Below: Medially the Tibia, laterally the Fibula.
- Patellar is the front “floating bond”
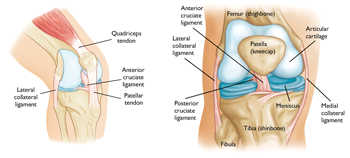
Ligaments:
- Anterior Crucial Ligament
- Posterior Crucial Ligament
- Posterior Menisco-Femoral Ligament
- Fibular Collateral Ligament
- Tibial Collateral Ligament
- Transverse Ligament (this one is visible only from the front side of the knee, below the patella).
In between the bonds we have:
- Medial Meniscus
- Lateral Meniscus
If this post is talking to you, book your next massage session by clicking here.
So, the knee joint can be divided into two parts:
- Tibiofemoral joint
Connects through the collateral ligaments, cruciate ligaments and menisci; - Patellofemoral joint
Gives stability to the medial and lateral retinaculum and allows the extension mechanism through the tendons of the quadriceps f..
Now that we have a better idea of what the knee anatomy is, we can look into his functionality.
Knee ROM are:
Extension: 0°
Flexion: 140°
Internal Rotation: 30°
External Rotation: 40°
Abduction/Adduction: 15°
Said so, we can see that the major movement that the knee can accomplish is, flexion.
Even if the Internal and External rotation since to be a big move for the knee, in the reality, that’s not always the case.
The older we get, easily this motion actively gets tighter.
Indeed, one of the main reason for meniscus injury is the twisting of the knee, when the feet is holding the ground and the body rotates.
But as previously mentioned in this post we would look into the knee special test.
What knee functional test have to tell us?
As we already mentioned in another post, a generic active, passive or resisted ROM tell us about muscle functionality.
On the other hand, a special test for the knee can show us if a ligament or a meniscus is loose, in the case of ligament or injured.
Furthermore, special tests, on the knee are essential to prevent further injury and reduce joint degeneration.
To start with we have the drawer test: Anterior Draw test and Posterior Draw test.
The Anterior one is to test the anterior crucial ligament, and the posterior, obviously, is for the crucial posterior ligament.
Both these tests are done with the client lying supine on the table, with a hip and knee flexed, and foot on the table.
The therapist will ensure that the foot doesn’t move and will place its hands around the knee, with the fingers (except the thumb) seating at the top of the calf and the thumbs seating on the patella.
For the A.D. test, the therapist will lightly pull the knee joint away from the patient body.
On the other hand, for the P.D. test, the therapist will push the knee towards the patient’s body.
These tests are positive if there is a loose movement within the knee, in the direction of pull or push.
If the client has a history of injuries, to the ACL or PCL the therapist wants to make sure not to push or pull with great effort, or injury could occur.

Vagus and varus test.
Those tests analyse the status of the medial and lateral ligaments.
For the valgus test, the therapist places one hand above the knee laterally, and the other hand above the ankle on the medial side.
By applying opposite pressure in the 2 directions we put the medial ligament under stress.
If pain is reproduced, or there is a loose movement the test is positive.
The same action is for the Varus test.
In this case, the hands are placed still above the knee and ankle, but the bottom hand is placed laterally and the top one, is placed medially.
Apleys Test
This test is used to evaluate the state of the meniscus.
The client, in this case, would be lying in a prone position, with the knee flexed.
The therapist will be standing next to the client, on the side of the knee flexed and will apply pressure to the knee.
If no pain is reproduced with pressure only, the therapist can gently apply a rotation movement to the flexed knee.
The test is positive if the pain is reproduced.
McMurray test.
This is luckily the most efficient and most used knee test used by therapists in case of meniscus injury
Here is how it works:
The patient lies in the supine position with the knee completely flexed (heel to glute).
Lateral Meniscus: the examiner then medially rotates the tibia and extends the knee.
Medial Meniscus: the examiner then laterally rotates the tibia and extends the knee.
McMurray is a positive test if the pain is reproduced.
There are still a couple of tests that can be done for the knee, but so far we did cover the most important.
About the therapy that I can offer for releasing knee pain, MLD is what I would suggest the most.
Especially for acute pain and swelling or oedema reduction.
Whereas, Myotherapy or Remedial Massage and Thai Massage can be used too but more to facilitate and or strengthen the muscle surrounding the area.