

Range of Motion is the movement of a joint within a 3-dimensional space.
For each joint, we expect a minimum and a maximum degree of movement.
When to use a range of motion evaluation.
Before performing a Myotherapy, Remedial Massage, or a Thai massage session, we check for a Range of Motion, also know as ROM.
Checking for ROM is to establish the functionality of the joint and the muscles that surround it.
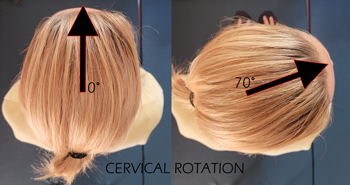
For example, when a client walks in complaining of cervical pain, the first thing we look in too after the postural assessment is the ROM.
A postural assessment is an evaluation of the skeletal structure.
After that, we ask the client to do specific movements with their head.
Like, Rotation side to side, flexion, extension, and lateral flexion.
Indeed, these are the basic range of motion for the cervical area.
What this range of motion can tell us?
Well, depending on the essential mobility of the person, we expect a minimum and maximum range.
Let’s say that the client has average mobility; we expect the range of motion of their cervical to be:
- Flexion (able to flex the head forward and leave a gap of 3cm between the chin and the sternum)
- Extension, we look in too 70° of movement
- Lateral Rotation we look in too 80° of rotation (the chin is nearly in line with the shoulder)
- Lateral Flexion we look in too 45°.
If this post talks to you, book your next massage session by clicking here.
Are the range of motion movements the same for everyone?
A person with a hypermobile joint range may have a 10° about less ROM than this.
Indeed, a person that has a hypermobile joint range can reach 10° furthermore.
That’s why every person needs his evaluation.
Moving forward, if the range of motion is limited, it could be a muscle tightness or a joint mobilization issue.
The best approach for improving joint mobilisation is the Myotherapy treatment or Thai Massage.
Both techniques relieve muscle tension and improve muscle tone and joint mobility.
The release of tension from the muscle would improve the ROM.
On the other hand, when we ask a client to do a ROM, we don’t look only for the length of movement.
Quality of movement.
For the quality of movement, we refer to how smooth the movement is.
Is the client trying to compensate for the cervical rotation by flexing the head?
Is the client compensating for the flexion by shrugging the shoulder?
Indeed, the movement of a joint is the key to understanding what muscle is responsible for the pain, discomfort or limited ROM.
Once we individualise the key muscle/s, we can address the issue.
Different types of ROM.
In conclusion, the ROM can be active, passive and resisted.
- The client itself does active ROM.
- Passive are ROM done by the therapist with no assistance in controlling the movement by the client.
- Reisted is ROM active done by the client, with a resistance force applied by the therapist again the client’s movement.
Each of this ROM can tell us something different about the joint.
Active is about muscle lengthening.
Passive is about joint mobility (ligament and tendon)
Resisted is about the strength of the muscle.
We can’t use the Resisted if Active or Passive reproduces pain. That would not be safe.
Regarding the Resisted ROM, the resistance is applied in 3 different levels.
When the pain gets reproduced, we stop the test.
Occasionally, an orthopaedic test can be performed too. Orthopaedic tests are specific tests to evaluate in specific the muscle involved in the limited ROM.