
Within the last few years, cosmetic surgeries have been on the rise in Australia. These types of interventions can be helpful for quick body changes. Still, the recovery process post-surgery is often under-estimated and misinterpreted, especially when, past a couple of days or just a few weeks, the body’s response to surgery leaves behind hard lumps, thick skin, and reduced sensitivity. The thought skin and lumps are simply fibrosis, and the reduced sensitivity results from damaged nervous system endings. At Melbourne Massage and Treatment in Fitzroy North, I specialise in Manual Lymphatic Drainage (MLD) using the Vodder technique, helping clients reduce swelling, assisting the recovery, and breaking down fibrosis post cosmetic surgery, safely and effectively. If you’re looking for post-surgery care in Fitzroy North or Melbourne, here’s how MLD can support your recovery and improve your results. What is Fibrosis After Cosmetic Surgery? Fibrosis formation post cosmetic surgery is the result of tissue damage that occurred during the surgery. When going for an intervention like liposuction, where fat is removed from the body (either at the abdominal level, arms or legs or elsewhere), the body, to replace the void left by the fat removal, builds up fibrotic tissue. The fibrotic tissue is mainly made of collagen. While this reaction is natural, it can often cause: Hard lumps or nodules under the skin; Uneven skin contour or texture; Tightness or restricted mobility; Tenderness or discomfort. There is no real way around those types of side effects post-liposuction, at least in the short term, and the body would take weeks to recover fully (up to 3 months). That said, everybody reacts differently to this type of intervention, and based on the type of intervention received, the recovery process can vary. Who Benefits Most From Lymphatic Drainage Massage After Cosmetic Surgery? Here is a short list of cosmetic surgery interventions that are going to leave you with fibrosis in the post-surgery time, and that would benefit from Lymphatic Drainage Massage intervention: Liposuction (abdomen, thighs, arms, chin) – This includes liposuction for Lipoedema management too. Tummy tuck – Either due to post-liposuction or from severe weight loss. Breast surgery (augmentation, reduction, reconstruction) – If this is due to breast cancer, one should be aware of any risk of Lymphoedema development. Facelifts and neck lifts Brazilian Butt Lift (BBL) – This type of intervention requires fat to be removed from other body parts, as the abdomen, and that’s where fibrosis would build up. How MLD Helps Reduce Fibrosis Manual Lymphatic Drainage (MLD) is a gentle, specialised technique that stimulates the lymphatic system to clear excess fluid, reduce swelling, and assist with the healing process. After surgery, your lymphatic system could be damaged and can struggle to keep up with its work, and that’s where MLD makes a big difference. Indeed, the stimulation of the Lymphatic System, via MLD therapy, can help in assisting your recovery and ensure that the fibrotic tissue gets absorbed and dismissed, restoring freedom of movement and leaving you soon after treatment in a deep relaxation state. I trained in the MLD with the Vodder style, therefore I can provide precise, tailored treatments that are safe for sensitive post-operative tissue. Book your post-surgery lymphatic drainage in Fitzroy North today to safely reduce fibrosis. When Can I Start MLD Treatment Post Cosmetic Surgery? Generally, MLD is safe to start as soon as the antibiotic cycle is ended post-cosmetic surgery. Given the light touch of this type of therapy, we aim to produce no pain during the treatment, so we can work close to the surgical side, without affecting the recovery process. On the other hand, I found myself occasionally referring patients to the local nurse or GP here at Fitzroy North Doctors, as their recovery immediately post-surgery was compromised by misleading suggestions and procedures offered by overseas cosmetic clinic surgery. If you are not sure about what’s going on with your recovery, please, before placing a booking for an MLD treatment, talk to your GP about your recovery state, and if you have any questions regarding MLD treatment, you can always reach out to me via the contact page. How Many MLD Sessions Do I Need To Reduce The Fibrosis? As mentioned earlier, everyone responds differently to cosmetic surgery, but in my experience, it would take at least 4 to 6 weeks to start seeing a significant difference in fibrous tissue presence. That said, the number of sessions and the time length of the sessions can vary, based on the area where you received the surgery. Abdominal surgery only: I will recommend 2 to 3 treatment per week, for the first 3 weeks. Within the first week, we may spend 1 hour per session, and from the 2nd week onwards, we reduce the treatment to 45 minutes. Multiple liposuction sites: as there are multiple areas where you received a surgery, we may need to extend the time of treatment up to 1 and a half hours initially, or go for multiple sessions, each for a different area. The first few treatment may take longer as we want to spend some extra time trying to break down the fibrosis with a gentler touch, due to the high sensitivity of the body, which is high due to post-surgery. As the sensitivity decreases, and we can apply further pressure, we can achieve the same result in fibrosis reduction with less time. If you are not sure what works best for you, you can book a 15-minute free online consultation, so we can discuss your needs and work out a treatment plan in accordance with them. MLD Prices in Fitzroy North All my services are offered at the same rate and are as follows: 90 mins – $175 1 hour – $125 45 mins – $ 115 30 mins – $90 All those prices are inclusive of GST. The 90-minute option is available only if required, and not via the booking system. Why Choose MLD at Melbourne Massage and Treatment in Fitzroy North? Not all lymphatic […]
Monthly Archives: September 2025
Blog
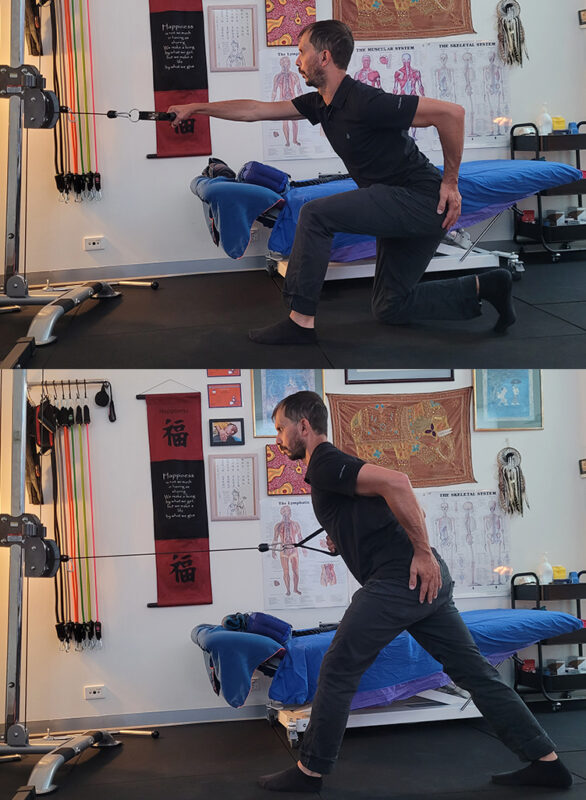
There Is No “Perfect” Lunge. Let’s Find Out Why.
While I guide my client during a 1:1 fitness class at Melbourne Massage and Treatment, [...]
Continue readingMar

Blog
Why the Gluteus Medius Is Essential for Balance, Longevity and Fall Prevention
One thing that can really create terror while we age is falling. No matter the [...]
Continue readingMar

Blog
Chronic Venous Insufficiency and Swollen Legs: Compression Is The Way To Go
In Australia, Chronic Venous Insufficiency (CVI) affect more women than men, with a ratio of [...]
Continue readingMar

Blog
It Is Never Too Late To Join A 1:1 Fitness Class
At Melbourne Massage and Treatment in Fitzroy North, as a clinical Myotherapist, I am enthusiastic [...]
Continue readingMar

Blog
MLD vs Lymphatic Massage: A Clinician’s Guide to What Works and Why
If you’re searching for lymphatic therapy in Fitzroy North, it’s common to see terms like [...]
Continue readingFeb

Sep
A pain response is a signal created by the brain to let you know that something within the body is not right, or at least, that something, potentially, is not right. This means that pain is a sensation that can also be there when no actual damage is present in the first place. But when you feel pain in the neck, in the shoulder, in the knee or somewhere, how can you differentiate if it is a pain given by muscles or by a joint? In this blog, I want to talk about the difference between muscle pain and joint pain. Muscle and Joint Pain: Let’s Start With Clinical History Intake When someone presents to the clinic in pain, the first thing I do is to track down their medical history, which includes their daily activities, previous injuries (old and recent), sports history, medications, quality of sleep, etc.. From there, I start to narrow down when they have been experiencing the pain, and what caused it in the first place, and where they feel it. Already, that information can give a good perspective of what we are looking at, in terms of muscle pain and joint pain. Knowing the time frame of the pain, the location of the pain can already give an answer. But before jumping to conclusions, we need to do some testing Active and Passive Movement: The Differences In Pain Response After an accurate intake of the clinical history, we would proceed with some testing, including active and passive range of motions. Active range of motions (AROM) are those movements that the patient would do on their own, like flexing the shoulder, rotating the hip, etc Passive range of motions (PROM), on the other hand, are movements that the therapist would do with the patient’s body. So you will be asked to keep your arm and shoulder relaxed, and it will be the therapist who moves the arm. Here is where things start to get interesting. If you respond with pain with AROM, we know that you are using both your muscle and joint to deliver the movement, so the pain response that you feel could be either from the muscle or the joint. But if you respond with pain with a PROM, then we know that the response is from the joint, because the muscle, in that specific motion, is not working. How about tendon? So, when delivering a PROM, we may push the movement to its limit, creating a stretch motion. This specific endpoint of movement, if it reproduces a really pinpoint specific pain, that is sitting right on to what we can recall as a tendon (the insertion point of the muscle), it is another differential tool to understand what the pain is caused by. So yes, to simplify, we use PROM to identify a joint pain, but in that joint pain, we include the tendon itself, not only the ligaments. Ligaments, per clarification, are the tissues that hold the bones together and make up the joint. Orthopedic testing: another tool for differentiating muscle pain from joint pain But the rabbit hole of understanding where that pain is from doesn’t stop here. That’s why we also use orthopedic testing when looking at a pain presentation. Ortopedic testing is a test that places stress on a specific structure, and can have a range of sensitivity and specificity. Sensitivity refers to the test’s ability to identify individuals who have the condition being tested for. Specificity refers to its ability to identify individuals who do not have the condition. Those two terms, that get evaluated in %, can tell us how valuable a test is. And most often, to validate a hypothesis of what can cause the pain, we have to use multiple forms of testing, from AROM to PROM to orthopedic testing and Clinical History. Neck Pain: Muscle Pain or Joint Pain – A case study Neck or upper shoulder pain is one of those common presentations, where the patient presents thinking that it is due to a muscle issue, but then, you prove to them that it is actually their joint that is the issue. Who is Peter, and with what pain does he present himself? Let’s examine a case study of Peter (name of fantasy), a 43-year-old office worker presenting with pain radiating from his right neck to the upper shoulder. Despite various stretches, the pain persists. He tried many pillows, he tried any sleep position, but this pain comes and goes, and has been on for years. Peter presents with a pain level today of 7/10, complaining that certain neck movements are limited and painful. It is hard, for example, to do a head check while driving. Clinical History So, first thing I would do is go through Peter’s clinical history and find out that his pain started about 10 years ago, after a whiplash accident, and that at that time, more than having a collar on his neck for a week or two, he hadn’t done much about it. Hi pain, which occasionally radiates to the neck, also gives him a headache. Sport history includes playing AFL from when he was a kid till his mid-twenties, and nowadays the occasional swim, yoga and pilates class. He spends most of his days working from home or at the office, sitting in a chair. In addition to this, we also know that: No pain radiating down the arms, no pins and needles in the hands; Pain is worst in the morning; Stretching gives an initial relief, but then it gets worse. Differential Diagnoses (DD) Differential diagnoses are the hypotheses we think of when someone presents with pain. Let’s say that is what we think we could find as a problem, given the patient’s complaint we received. And out of 3 or 4 DD’s, we will draw a line that connects all the results and get a Working Diagnosis (WD), which is the most plausible answer given the results we obtained. This said, this […]