
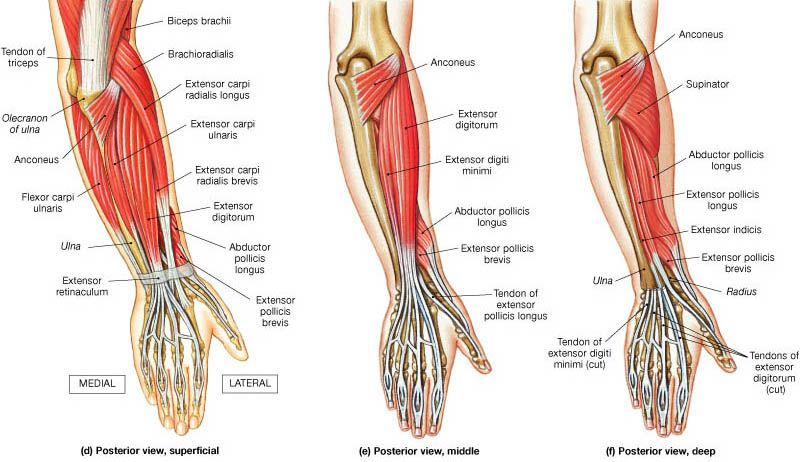
Elbow tendinopathy, whether it presents as tennis elbow (lateral elbow pain) or golfer’s elbow (medial elbow pain), is one of the most common overuse injuries in active people, desk workers, and manual labourers. At Melbourne Massage and Treatment in Coburg, I frequently help patients recover from both forms of elbow tendinopathy. Elbow Tendinopathy: How Does It Manifest? “Tendinopathy” refers to irritation and degeneration within a tendon due to repeated overload. Elbow Tendinopathy, in both of its forms, tennis or golfer’s elbow, can sound like a sport-related injury, but it has little to do with the sports world. The reason why those presentations carry their name is due to the sport action, which requires that specific muscle group to work to deliver the golfer strike (medial) or tennis strike (lateral). So what can actually cause an elbow tendinopathy are: Sudden increase of tendon load – lifting heavier than usual, at the gym or at work Repetitive action – think of that constant mouse or keyboard action in the office environment Overstretching of the tendon – Poor office ergonomics can overload the elbow joint and the elbow’s tendons To be more specific, the office worker presenting with elbow tendinopathy often has repetitive mouse/keyboard use, which is often accompanied by poor ergonomic factors, such as the forearm being in a prolonged pronated position (palm facing down), which places the common extensor digitorum tendon (CEDT) under stretch. Medial and Lateral Tendinopathy of the Elbow Let’s look into the difference between the actual Tennis (lateral) and Golfer’s (medial) Elbow. Tennis Elbow (Lateral Epicondylitis) Pain in the outer elbow Irritation of the wrist extensor tendons, especially the Extensor Carpi Radialis Brevis (ECRB) Familiar with typing, lifting, racquet sports, and DIY tasks Golfer’s Elbow (Medial Epicondylitis) Pain in the inner elbow Irritation of the wrist flexor tendons Related to gripping, pulling, forearm rotation, and throwing How To Recover From a Tendinopathy? Despite different pain locations, the rehab approach is almost identical, and while rest provides temporary relief, it does not fix the underlying tendon changes. The true solution? A structured, progressive exercise rehab program that restores tendon strength and resilience. In fact, as the tendinopathy itself came to be an issue due to an overload of the elbow’s tendon, to settle the pain and discomfort, we have to: Reinforce the elbow tendon and muscle so that it can perform better. Analyse what overloaded the elbow tendons – we have to understand what can be changed in the loading process, starting from: Shoulder stability (looking up in the joint chain – Mobility and Stability) The ergonomic of your workload, that is, office or heavy repetitive work (like gardening, for example, or construction). Workout program – ensure there is a progressive load in the program that is right for your capacity. The 3-Phase Exercise Program for Elbow Tendinopathy Here at Melbourne Massage and Treatment in Coburg, as a clinical myotherapist, I get to see many patients presenting with Elbow Tendinopathy, and the rehab protocol and recovery that I used is detailed below. Phase 1: Pain Reduction & Tendon Activation (Week 1–3) In this initial phase, the goal is to calm symptoms without resting the tendon completely. Tendons respond best to gentle, controlled tension, better known as isometric exercises. Isometric is ideal because: Tendons have a low blood supply compared to muscles, so in order to receive the nutrients that allow the healing process to be delivered, they need long and steady engagements. A tenodon that is inflamed presents with disorganised collagen fibres, which are not running straight, and no longer form a compact line. And there is a need for a constant load to restore new fibres that can regain the tendon’s functionality. Wrist Extension Isometric (for Tennis Elbow) You will be sitting at a desk with your forearm comfortably supported by the desk, with your hand in a prone position (palm down) Slightly extend your wrist against resistance. Pain-free movement (it could be a bend or a lightweight) Hold 20 seconds, repeat 10 reps Wrist Flexion Isometric (for Golfer’s Elbow) You will be sitting at a desk with your forearm comfortably supported by the desk, with your hand in a supine position (palm up) Deliver a slight wrist flexion against resistance. Again, it has to be a pain-free movement. Hold 20 seconds, repeat 10 reps Time of hold, repetition and pain response are subjective to each individual. That’s where we would stop and focus on each individual clinical history and presentation, and adapt the elbow tendinopathy rehab program to your needs. Gentle Mobility & Dry Needling From a point of view of massage for elbow tendinopathy, there are a few techniques that work really well, especially in the early phase of recovery: Joint Mobilisation – passive movement applied to the wrist and elbow joint, to improve the range of motion of this joint and disengage the area. Dry Needling – The usage of a needle on muscle, to create a micro-inflammation and to drive more attention from the nervous system into the targeted area. Deep Tissue Massage – When dry needling is not an option, deep tissue massage can also help in creating this targeted central nervous system response. Phase 2: Strength & Tendon Remodelling (Week 3–8) This is the most critical phase, and the one that actually restores tendon health. Eccentric Wrist Extension (Tennis Elbow Gold Standard) How to do it: Extend the wrist of the affected side with your good hand, while in the affected side, you are holding a lightweight or resistance band. Slowly lower the weight with your injured side with a tempo that last 3–5 seconds Repeat 12–15 reps, 2–3 sets – this is an endurance setup. Between each set, rest for at least 30 seconds. Eccentric Wrist Flexion (Golfer’s Elbow Gold Standard) Same method, but applied in a flexion motion. Assist the initial movement of flexion Slowly bring the wrist back to the straight position with a 3-5 second tempo. Look always at somewhere between 12-15 reps, for endurance performance. The eccentric […]
Tag Archives: Dry needling

Blog
Why I Chose Coburg for My Myotherapy Clinic
I had been looking for a new space to relocate my Myotherapy Clinic, and when [...]
Continue readingJul
Blog
Lipalgia Syndrome or Lipoedema? Why the Name Matters
Lipalgia Syndrome is a name for a condition that most often, and more commonly, we [...]
Continue readingJul
Blog
Melbourne Massage and Treatment Is Returning to Coburg in July 2026
After two wonderful years in Fitzroy North, I am now ready to announce that Melbourne [...]
Continue readingBlog
When You Should Stop Running? And For How Long?
Here at Melbourne Massage and Treatment, Myotherapy Clinic in Coburg, when treating patients who love [...]
Continue reading
Blog
Pillow For Neck Pain: What You Need To Know
When treating someone for neck pain, a common question I get asked is: “Should I [...]
Continue readingJun

Oct
Exercise is the ultimate medicine for longevity and well-being. That said, there are different ways to exercise, and you should choose which one based on your goals and needs. Ultimately, even if you will prioritise one type of exercise over others, training in different ways, it is the best option to build resilience, strength and obtain the best results. But what are these main ways of training? Well, in this blog, we are talking about Strength Training and Hypertrophy. At Melbourne Massage and Treatment in Coburg, I help people achieve this goal, with tailored injury recovery Myotherapy plans that may start with hands-on treatment but aim to get the person moving and moving under load. What Is Strength Training? Strength training, in its pure form, is a type of training that aims to improve the body’s ability to produce maximal force. This is possible by optimising the nervous system’s capacity to communicate to the muscles what action has to be delivered when placed under load. In fact, the goal isn’t necessarily to make muscles bigger, but to make them stronger. Here is a breakdown of what a strength training session would be like: Typical rep range: 1–6 repetitions per set Load: Heavy (80–100% of your one-rep max) Rest periods: Longer (2–5 minutes) Primary outcome: Improved neural efficiency — your brain and muscles learn to work together more effectively. This type of training benefits everyone, from athletes to everyday movers, by: Enhancing joint stability Improving bone density Increasing functional power for daily tasks. What Is Hypertrophy Training? Now, we will examine another form of training that aims to increase muscle size. Indeed, hypertrophy focuses on creating controlled muscular fatigue that stimulates growth in the muscle fibres. Here’s how it works: Typical rep range: 6–12 repetitions per set Load: Moderate (60–80% of your one-rep max) Rest periods: Shorter (30–90 seconds) Primary outcome: Increased muscle cross-sectional area (growth). Hypertrophy is popular for aesthetic goals, but it also has significant benefits for: Joint support Posture Injury prevention, especially when paired with proper mobility and recovery practices like myotherapy. Who Would Benefit from Strength and Hypertrophy Training? Let’s be clear that both styles of resistance training can benefit a wide range of people — not just athletes or bodybuilders. But here is a clearer breakdown of which training belongs to which goals: You’ll benefit from strength training if you: Want to improve performance in sports or daily activities that require lifting, pushing, or pulling. You are seeking to increase bone density and joint stability, especially as you age. This is a big one for menopausal women. Need to enhance posture and core control to reduce the risk of back or shoulder pain. Are recovering from injury and looking to restore functional movement patterns safely under guidance. You’ll benefit from hypertrophy training if you: Want to build muscle mass for aesthetics, strength, or body composition. You are addressing muscle imbalances or weaknesses identified during myotherapy assessments. Need more joint support and stability through improved muscular structure. Aim to boost metabolism and energy expenditure through increased muscle tissue. At Melbourne Massage and Treatment, I often integrate tailored exercise advice with fitness class sessions, helping clients find the right balance between strength, mobility, and recovery for their individual goals. Massage Therapy, Dry Needling, and the Role of Passive Treatment Massage therapy, dry needling, and other forms of passive therapy are valuable tools during the recovery phase of an injury or when pain and tension are high. They help by: Reducing muscle tension and spasm Improving blood flow and assisting with tissue healing Calming the nervous system and reducing protective muscle guarding Restoring short-term mobility to prepare the body for movement At my Coburg clinic, these treatments are often used early in a client’s recovery journey to reduce pain and restore comfort. However, while these therapies are excellent for short-term relief and acute recovery, they must eventually be paired with movement under load to create lasting change. Why Movement Under Load Is Essential for Long-Term Wellness Passive treatments can help you feel better, but loaded movement enables you to function better. When you progressively load muscles, tendons, and joints, your body adapts and becomes stronger and more resilient. This is what keeps pain away in the long term. Here is a practical and simplified explanation: “You have to think that the body, while it does age, it does slow down in any form of its metabolism, including the regeneration of tissues, which gets worn down, and finds it difficult to be regenerated. This is where movement under load plays a crucial role. Movement under load indeed, it is the stimulus that the central nervous system needs to maintain the body’s regeneration active and effective”. A further breakdown of why movement under load matters beyond recovery: Builds tissue resilience: Strengthens muscles and connective tissue to handle daily demands. Supports nervous system retraining: Teaches your body to move efficiently and safely. Improves joint health and posture: Strengthens stabilising muscles that protect joints. Reduces recurrence of pain: Prevents the same issues from returning by addressing root causes, not just symptoms. Another way I would express the difference between passive therapy and exercises (under load) to my patient is: “Massage and needling help you feel good now, but movement under load helps you stay good later.” That’s why our approach combines hands-on therapy to relieve pain with movement education and strengthening to keep you moving well long after your treatment. How Myotherapy Complements Strength and Hypertrophy Training Myotherapy is a form of manual therapy that aims to improve the performance of any individual who has gone through an injury or someone who wants to maintain functionality and wellbeing. In a Myotherapy session, we would start with some form of testing to evaluate the person’s capacity in mobility and strength and from there we create a treatment plan that aims to improve the current presentation. A treatment plan may include: Soft tissue therapy Corrective exercise Movement assessment Goals of myotherapy: Address muscular imbalances from repetitive […]
I did stop counting the number of times I hear patients say that their hamstrings are tight, and that’s why they can’t bend forward. And I did stop counting, because this happens so often that it is really hard to find someone who actually knows what tissue is limiting their movement. In fact, most of the time, what is happening is not hamstring tightness, but rather a lack of hip hinging and associated hip mobility, or neural tension (in this case, the sciatic nerve neural tension). What Is Neural Tension? When we discuss neural tension, we refer to the lack of mobility of the nervous system’s connective tissues, so the actual nerve as a fibre or tissue, when it’s put under mechanical stress (like tension, compression, or stretch). Here is an example: When we bend forward, the sciatic nerve (the largest nerve in the body) runs from the lower back (Ventral rami spinal nerve L3-S1), through the buttocks (below the piriformis muscle most of the time), and down the back of the leg (right between the hamstrings muscles). When doing such an action, the nerve needs to glide freely, and if any where along its journey, there is a compression, due to other tissue tightness or inflammation, or even a physical outer pressure (a belt from the pants) it becomes irritated, compressed, or “stuck” ending not moving well. That’s where you may experience a pull on the back of the leg. That is neural tension. More specifically, your symptoms can be: A deep pulling or burning stretch in the back of the thigh or calf. Tingling or numbness (especially if holding the stretch for a longer time) A sensation of “snapping” or “tugging” deep in the leg when stretching Limited range of motion that doesn’t improve with traditional hamstring stretches How Is Neural Tension Different from Muscle Tightness? While neural tension and muscle tightness may feel similar, they are fundamentally different in their causes and treatments. Muscle Tightness Neural Tension Origin Muscle fibres are shortened or tense Nerve or nerve sheath is restricted or irritated Sensation Broad stretch, fatigue, cramping Sharp, burning, electric, or pulling sensation Area Felt Localised to the muscle belly Along a nerve pathway (e.g., back of the leg) Improved by Stretching and massage Nerve gliding/mobilisation, reducing irritation Common in Athletes, post-exercise, poor posture Sciatica, herniated discs, hipo-mobility, and a sedentary lifestyle Now, Let’s Talk About Forward Bending When bending forward with the upper body, aiming to reach the toes or the floor with the hands, we may experience a stretch in the back of the leg. That stretch it may not be only your hamstrings but also the sciatic nerve. When this nerve lacks mobility, as expressed earlier, due to things like disc issues, facet joint irritation, piriformis syndrome, or general irritation, it can feel like your hamstrings or calf or back are tight, even when they’re not. A good way to understand if the feeling of tightness is from your nerve or not is to perform a Slump Test. How to perform a Slump Test? Below is a step-by-step guide on how to perform the slump test: Sit on a chair or table, where both feet are off the ground; Slump your body forward, while looking straight ahead, and your arms are crossing behind your back (which means your spine rounds backward, your shoulder drops forward); Now, start lifting up one leg, while the other one is bent at the knee at 90°; While you lift up the leg, start noticing if you feel any pulling sensation from the lower back going down to the back of the leg or calf (it could be anywhere along the lower back to the feet); If you manage to reach full leg extension, now, start looking down (you may notice tension arising or increasing); If nothing happens yet, then bring your toes (of the leg raised) backwards (ankle dorsiflexion); If, along any step of this process, your pulling sensation increases (more intense) or becomes longer (like from only the back of the leg, it now feels even in the back or in the calf), this is neural tension. Indeed, the tension would feel like a long rope pulled across multiple joints (lumbar, hip, knee) with a burning sensation and maybe some pins and needles. Next, to experiment further with the neural tension, start looking up with the head, go if you can in full cervical extension, and you should feel relief in the back of the leg tension. This last step is proving to you how, by releasing the central nerve (that travels in the central canal of your spine), the neural tension slows down. You are stopping the nerve’s pull from its origin, the brain. Should You Stretch a Nerve? No, not really. Nerves aren’t designed to be stretched like muscles. In fact, if you keep stretching a nerve aggressively, you may end up irritating the nerve and worsening the symptoms. Instead, use nerve gliding or joint mobilisation exercises, which are gentle, rhythmic movements that help the nerve move through its surrounding tissues without overstressing it. And to stay in the loop, let’s look at the sciatic nerve glide: Lying on your back, lift one leg while keeping the knee slightly bent. Slowly extend the knee and flex the foot back toward you, then release. Repeat in small, pain-free ranges. This can help restore nerve mobility without aggravating the nerve. If this is not the case, and you still experience pain and discomfort, then it is probably time to book an appointment (myotherapy) to ensure there is not significant entrapment along the nerve pathway, and see what can be done to relieve that compression. How Myotherapy Can Help with Neural Tension? As a Clinical Myotherapist, I specialised in assisting people with any sort of musculoskeletal issue. Neural Tension is one of those. During a Myotherapy session, we would address, via a detailed clinical history and a series of assessments, what may be the cause of the neural […]

May
As a Clinical Myotherapist, I often work with patients who perform back squats as part of their exercise routine, and at the question: “What’s your goal with a back squat?” the answer is often vague and not specific to what this exercise is for. The reason why the answer is not specific is simply because they don’t know what the difference is between high and lower bar squat, and don’t know that the back squat, as long as it is an amazing functional movement, doesn’t train all the lower body muscles at the same level. That’s where, to prevent injury, to perform better squats, and to strengthen more evenly all the lower body muscles, I would suggest them to do exercises like: Quads curl, Hamstring curl, Cable Machine Adduction and Diagonal Extension (Glute Medius). Back Squat: The Foundation of Strength The back squat is such a great form of exercise because it trains multiple joints and multiple muscles all at once, but also allows us to use our innate capacity of squatting, which is a functional movement, to move high loads, therefore achieving more strength gains. However, this leaves us with more responsibility to train smartly. So let’s start to break down the two main types of back squat: High-Bar Back Squat (Upper Bar Position) The bar rests on the upper traps The torso remains more upright Greater emphasis on the quadriceps muscles Ideal if your goal is quad strength and knee-dominant movement patterns Ideally, you are standing with your heels elevated from the ground The fact that the bar is sitting on the upper traps, and that the torso sits straighter, would lead to a descending movement where your back thigh (hamstrings) would lean on calf muscles, and from there you will stand back up. This is why you put more force throughout the quads. Indeed, the combination of a higher bar, a straighter torso, and a reduced descending position allows the weight to sit in the middle of the centre of gravity, which is placed more posteriorly than in a lower-bar back squat. Low-Bar Back Squat (Lower Bar Position) Bar rests lower on the rear deltoids Torso leans forward slightly more Greater load on the glutes and posterior chain Favoured by powerlifters Best for developing hip strength and glute activation Ideally, your feet are nice and flat on the ground from heel to toes. On the other hand, the lower-bar back squat, as anticipated, is more for the posterior chain muscles, like the gluteus max. This is possible because the bending forward of the trunk stretches more muscle fibres in their origin point (the posterior aspect of the ilium (the pelvic bone), the sacrum, and the coccyx), allowing more fibre contraction in the ascending movement. Also, the lower position of the bar and the bending of the torso maintain the weight in the middle of the centre of mass, which is pushed forward at this time. How about if I cannot squat deep? The depth of a squat is the distance that you can cover from a standing position to the lowest point you can reach. How deep you can squat will definitely change which muscle groups you can activate, but not everyone can squat deep —and that’s absolutely ok. Each of us has biomechanics that are different, due to differences in how the skeleton is shaped. Without going into many details in this blog, we can definitely say that those who have a longer femur would have a harder time going for a deep squat, compared to those who have a shorter femur. The femur’s length is compared to that of the torso. But this is not all, indeed, there are also other femur and hip characteristics that can limit how deep you can squat, such as an anteverted or retroverted femur head. Other conditions that can get in the way while you squat are hip impingement. Accessory Work for a Complete Lower Leg Program So, knowing when and why to use each back squat variation can help tailor your program toward specific goals or help rehab muscle imbalances through focused intent. No squat is right, no squat is wrong; it is all about your goal. However, we need to add work more specifically with other exercises for strength symmetry, muscle activation, and injury prevention. Quad Curl (Leg Extension) Isolates the quadriceps Improves knee tracking and squat depth Essential in rehab for knee pain or quad weakness Quads curl can be done in many ways, with a cable machine or on a bench with a quads curl attachment, but even with a kettlebell or resistance band. It all depends on your setup. As per all the exercises, be consistent with your set-up and progressions. What I prefer most for my training, and what I offer to my patients during the fitness class, is to do quad curls on a bench with the attachment for quad curls. The advantages of this set-up are: Confort Easy progressions Easy set-up Inclination of the back at about 45° to 65° and slight elevation of the quads. The last point is essential to ensure we engage both ends of the quadriceps femoris, which is one of the four quads, that crosses both the hip and knee joints. Hamstring Curl Focuses on the hamstrings, which during a squat are often undertrained Strengthens the back of the thigh and supports knee stability A must-have for runners and athletes prone to hamstring strains As per the quad curl, even the hamstring curl can be done with different variations; there is never one way to train those muscles, but again, it is all about the efficiency and the amount of load that we can put through the muscle, which makes a difference. And again, what I can offer at Melbourne Massage and Treatment, in Coburg, is to do these exercises on a bench, using this time a lower inclination for the upper body (which is now in a prone position) so that the origin of the […]

May
The Star Excursions Balance Test (SEBT) is a fabulous functional test that can tell us a lot about the mobility and stability of the ankle, knee, and hip joints. On top of being a functional test, the star excursion can also be used as an exercise, and via a series of progressions, which we will discuss in more detail later, can help you train for better running performance and injury prevention. Why is the Star Excursion Balance Test Important? The importance of the Star Excursions Balance Test lies in its ability to assess, with one motion, the capacity of your ankle to remain stable on the surface of support (the floor) and how this stability is transmitted to the knee first and, consequently, to the hip. This is possible because the transfer of vertical pressure is applied to each joint while you are aiming to get the movement done. The movement required is to keep the feet of the anchor down to the floor, from the toes to the heel, while with the other foot, you aim to reach the furthest point away within the eight cardinal directions (like a star *). Along those movements, then, we also get observational data about your: Proprioception: The ability to sense the position of the body and its parts in space. Balance: The ability to control the body’s centre of mass over a stable base of support. Functional Movement: How well the body can perform multi-directional movements, such as stepping, reaching, and stabilising. The Role of the Star Excursion Balance Test in Lower Limb Injury Recovery So, if you are someone who has sustained lower limb injuries, particularly around the ankle, knee, or hip, these capabilities are often compromised. By using the Star Excursion Balance Test, we can: Assess any deficits in these areas, which might increase the risk of re-injury or limit recovery progress. But not only that. Indeed, that information will shape the recovery program, allowing us to understand better which muscle group or joint we need to focus more on with the exercises. Help runners, as running is a dynamic activity that places high demand on the lower extremities. Even minor imbalances or weaknesses can lead to conditions such as IT band syndrome, shin splints, and knee pain. The Star Excursion Balance Test helps in identifying these early warning signs before they evolve into more serious conditions. What Does the Star Excursion Test Measure? The primary purpose of the SEBT is to evaluate a person’s capacity to control body movement while standing on one leg. In rehabilitation, the Star Excursion Balance Test trains and improves: Ankle Stability and Control: It challenges the ankle to support the body’s weight while shifting through various planes of motion. Knee and Hip Joint Function: By demanding strength and flexibility in the lower limb, it helps retrain the kinetic chain, especially after joint injury. Balance and Proprioception: The test improves your ability to sense where your body is in space, which is essential for both preventing and recovering from injuries. Postural Awareness: Training balance also trains your ability to maintain proper posture, which can reduce stress on your joints and muscles during exercise. In fact, the test consists of reaching with one leg in multiple directions (anterior, posterior, medial, and lateral and a mix of those directions) while maintaining balance on the other leg. This shows their neuromuscular control and postural stability. It mimics the demands placed on the body during dynamic activities like running, cutting, and jumping. The Progression of the Star Excursion Test The beauty of the Star Excursion Test is its flexibility. It can be adapted based on the individual’s injury level, fitness, and goals. The test itself involves several variations, which I implement depending on the stage of recovery or the individual’s needs: Softer Ground: For those in the early stages of rehabilitation, we may perform the test on a softer surface, such as a foam pad or balance disc. This reduces the stability of the base and forces the individual to engage more stabilising muscles, which aids in proprioceptive training and can be beneficial for rebuilding ankle and knee control. Weight on the Ankle: For those who have had ankle injuries, I often modify the test to place more weight on the injured ankle. This helps rebuild strength and functional control, as it forces the injured area to bear load and engage in movement patterns that may have been avoided during the healing phase. Eyes Closed: To increase the challenge, I sometimes ask my clients to perform the test with their eyes closed. This removes visual input, forcing the body to rely more on internal feedback (proprioception). This is especially important in the latter stages of rehabilitation, as it helps to refine neuromuscular control and reduce reliance on external cues. Using the Star Excursion Test with Lower Limb Injury Recovery and Runners The SEBT is a functional test that I like to use, with all its variations, to assess the progress of patient recovery. Whether you present with an injury, or you want to improve your form and body functionality throughout exercises, the SEBT allows us to look in depth at what we need to work on, too. For example, after a sprained ankle, I’ll often use the SEBT to check whether an individual is able to move without compensation, ensuring that their body has regained sufficient control and strength before returning to activities like running or sports. And this, don’t be surprised, is something that I do and has to be done whenever someone presents with complaints about knee or hip pain, too. Again, an unstable ankle would transmit that instability up the chain. On the other hand, for runners, the test helps evaluate areas of weakness that might predispose them to injuries such as Achilles tendinopathy, patellofemoral pain, or iliotibial band syndrome. Since running places repetitive stress on the lower limbs, identifying and addressing weaknesses early can prevent long-term problems and improve overall performance. Myotherapy and SEBT […]

May
Muscle tension headache and migraine are two different types of presentation that have in common a pain, which can also be debilitating, in the head area. Back in 2019, in Australia, 3 million people were estimated to suffer from migraine (Wijeratne et al., 2023), where, define how many people are suffering from muscular tension head-ache is a bit more tricky, as is not a presentation that can be easily tracked, due to self managed protocols, and other miss data counting. That said, they have different origins, symptoms, and treatment options. In this blog post, we will explore the key differences between muscle tension headaches and migraines, helping you understand how to identify and manage them. What Are Muscle Tension Headaches? Muscle tension headaches, or tension-type headaches, are the most common. This type of headache originates from cervical or facial muscle tensions, which recreates a pattern of pain on the head of facial area. As with all muscles, but even joints, the pain that we can experience can be local or in an area around the tense spot. These headaches are often linked to stress, lack of good posture, anxiety, and even sleep disturbances. They can be chronic or occasional, but compared to migraine, they lack neurological symptoms. Symptoms of Muscle Tension Headaches: Dull, aching pain or pressure around the head, especially in the forehead, temples, and back of the head. A sensation of tightness or “band-like” pressure around the head. Mild to moderate intensity (usually not as severe as a migraine). Pain can last from 30 minutes to several hours, sometimes even days. Tenderness or tightness in the neck, shoulders, and scalp. Causes of Muscle Tension Headaches: Stress: Emotional and mental stress is one of the primary causes of muscle tension in the neck and scalp muscles. Lack of good posture: Sitting or standing with poor posture and lack of strength in the musculoskeletal system, especially for long work, can strain muscles and trigger headaches. Sleep issues: Sleep deprivation or poor-quality sleep can exacerbate muscle tension and lead to headaches. The body recovers from the fatigue of the day before during sleep, especially in the early morning hours. Sleep deprivation would increase the chance of a headache. Dehydration: Not drinking enough water can lead to tension and headache symptoms. The body withdraws water from the brain to keep the organ functioning, causing physical brain shrinkage, which leads to headaches. Recent studies have indicated that chronic tension-type headaches (CTTH) are often exacerbated by environmental stressors, and poor posture in daily activities can cause muscle imbalance and contribute to the frequency of these headaches (Bendtsen et al., 2018; Grazzi et al., 2016). Treatment Options: Pain relief: Over-the-counter pain relievers, like ibuprofen or acetaminophen, can help ease the discomfort. Heat pack: Applying a warm compress to the neck and shoulders can help relax tense muscles. Keep always in mind that heat application should be limited to 10-15 minutes, once or twice a day. Massage: Gentle massage of the neck and shoulder muscles can reduce tightness and alleviate headache symptoms. Stress management: Practising relaxation techniques such as deep breathing, thai yoga, and meditation can reduce stress and prevent muscle tension headaches. Strengthen muscles: Strengthening the muscles around your cervical and shoulder area can help reduce the chance of suffering a headache by reducing the inflammatory response that the muscle would activate due to a lack of strength. What Are Migraines? As I mentioned above, the significant difference between headaches and migraines is due to neurological symptoms, a unique characteristic of migraines. Migraines are neurological events that involve complex brain activity. They are characterised by intense, throbbing pain, usually on one side of the head. They are often accompanied by other symptoms such as nausea, vomiting, and sensitivity to light and sound. Migraines are more debilitating than muscle tension headaches and can last a few hours to several days. The intensity of the headache doesn’t have to be severe. Symptoms of Migraines: Although many people experience nausea, vomiting, and light sensitivity, migraine symptoms can vary, with some individuals experiencing dizziness or visual disturbances without significant head pain. Throbbing or pulsing pain, usually on one side of the head. Nausea and vomiting. Sensitivity to light, sound, and sometimes smells (aura). Visual disturbances such as flashing lights or blind spots (this is known as an aura, which can occur before or during the headache). Dizziness or feeling lightheaded. Migraines are understood to be primarily driven by neurovascular changes and neuronal hyperexcitability (Feng et al., 2021). A review by Wagner et al. (2021) found that the pathophysiology of migraines involves alterations in neurotransmitter systems, notably serotonin and CGRP (calcitonin gene-related peptide), which contribute to the vasodilation and pain signaling pathways. Causes of Migraines: Genetics: Migraines tend to run in families, suggesting a genetic component. Hormonal changes: For many women, changes in estrogen levels, such as during menstruation, pregnancy, or menopause, can trigger migraines. Environmental triggers: Bright lights, strong smells, certain foods (like chocolate, cheese, or caffeine), weather changes, lack of sleep, and allergies that cause sinus issues are common migraine triggers. Neurological factors: Migraines may involve changes in the brain’s nerve pathways, chemicals, and blood vessels, which cause inflammation and pain. Treatment Options for Migraines: Prescription medications: Triptans and anti-nausea medications are commonly prescribed to treat the acute pain of migraines. Preventive medications: For frequent migraine sufferers, medications such as beta-blockers, antidepressants, or anti-seizure drugs may be prescribed to reduce the frequency and severity of attacks. Lifestyle changes: Regular sleep, a healthy diet, and consistent exercise can help reduce the frequency of migraines. Cognitive-behavioural therapy (CBT): Managing stress through therapy can help alleviate migraine triggers. Alternative therapies: Acupuncture, biofeedback, and massage therapy are sometimes used as complementary treatments for migraine management. Recent studies support preventive treatments for chronic migraines, such as CGRP antagonists (Kundera et al., 2020) and neuromodulation techniques like transcranial magnetic stimulation (Lefaucheur et al., 2017). Key Differences Between Muscle Tension Headaches and Migraines Although muscle tension headaches and migraines involve head pain, they differ […]

Mar
Bone density is a key factor in bond fracture prevention. Bone is made of cells that die and regenerate. When this process is compromised, the risk of fracture arises. During the early stages of life, we can ensure that we intake and store calcium through food to build up our bones, but after a certain age (about 30), the body stops absorbing calcium, and the storage that we created is now our reserve for the rest of life. Cell Regeneration in Bone and Other Body’s Tissues The body’s cells, like muscle cells, skin cells, tendon cells, ligament cells and even bond cells, are in constant change via a process called cell regeneration. Old cells die off and they get replaced with new cells. In the case of bone, the cells that allow this process to happen are called osteoblasts. While we age, this process slows down, meaning that cells would still die, but they don’t get replaced. A typical example is a woman going through menopause. Estrogen, which is the hormone responsible for bond metabolism, allows the activity of osteoblasts. During menopause, indeed, women have a drop in Estrogen production, and osteoblasts are not as operative as they used to be. Strength Exercises and Cell Regeneration As this meta-analysis shows, strength exercises are a positive stress stimulus for the body and can help the osteoblast work harder and maintain bone cell regeneration. When the body perceives stress as physical resistance, it does its best to establish a reparation mechanism. So whenever we pick a weight against gravity, the body would implement a regeneration of the tissue that are used to complete this action. Who Is at Risk of Losing Bone Mass? There are several factors that can contribute to decreased bone mass: Age: Bone density typically peaks in early adulthood and declines with age. Gender: Women, especially postmenopausal, are at higher risk due to hormonal changes that accelerate bone loss. Family History: A family history of osteoporosis can increase risk. Body Size: Individuals with smaller body frames may have less bone mass to draw from as they age. Hormonal Levels: Thyroid imbalances and reduced sex hormones can lead to bone loss. Dietary Factors: Low calcium and vitamin D intake contribute to diminished bone density. Lifestyle Choices: A sedentary lifestyle, excessive alcohol consumption, and smoking are linked to weaker bones. I have included factors like dietary and hormonal levels in the above list. Bear in mind that taking supplements such as calcium and vitamin D (which helps retain calcium) could have severe contraindications. So, always talk to your doctor or specialist about the intake of supplements. How to determine Bone Density? To determine bone density, there is a diagnostic test called Dual-energy X-ray Absorptiometry (DEXA or DXA). This non-invasive procedure measures the mineral content in bones, usually in areas like the spine, hip, or wrist, to assess bone density and identify potential risks of osteoporosis or fractures. The results are given as a T-score, which compares your bone density to the average peak bone mass of a healthy young adult. A T-score of -1.0 or above is considered normal, while a score between -1.0 and -2.5 indicates low bone mass (osteopenia), and a score of -2.5 or lower suggests osteoporosis. Other methods, like ultrasound or quantitative computed tomography (QCT), can also assess bone density, but DEXA remains the gold standard for bone health evaluations. Mobility before strengthening So far, we have discussed how strength exercises are a good way to maintain bond density. Still, I would not recommend that anyone who is not into strength exercise and has bone density issues go and start lifting heavily. Why (?), you may ask. Well, before we start lifting heavy, we want to ensure that the body mechanics are optimal for it, so we better start looking into your mobility and then pass on to the strength part of things. Please be aware that mobility has nothing to do with elasticity or stretching. Those are different practices. How Can We Achieve Great Mobility For people who decide to take a journey to ensure an optimal level of mobility and then strengthen the body, the first step is to assess their joint mobility with active and passive range of motion. After that, we could use a combo of Myotherapy treatment and mobility exercises to ensure they can quickly pick up the best of their mobility capacity, given their subjective presentation. And here is a list of mobility exercises which we may look into at first: Hip Openers to improve range of motion in the pelvis and lower back. Ankle Drills to support proper weight distribution in weight-bearing exercises. Thoracic Spine Mobility Exercises to prevent excessive strain on the lower back. AC Joint External rotation to ensure we can build strong rotator cuff muscles, essential for shoulder health It Is Time To Strength. How Can We Do This? Once the minimum mobility is achieved, which may take 1 to 2 weeks of training, depending on each individual and their subjective history and effort, we can start looking into more strengthening exercises. So, here is a list of different exercises that can help with strengthening, written with the progressions to follow: Calf raises with double leg, single leg and weight Hamstring and Quads Curl that gets weight added as weeks go by Standing Adduction and Abduction at cable machine or with resistance bend Glut Muscles training at cable machine or with resistance bend Deadlift for back and posterior chain muscle strength Squat with weights and explosion variations Cuff rotator-specific strength is Ideal before stepping into more complex arm weight-lifting Cervical muscle strength to prevent cervical headache and sore neck All of those exercises, except the cervical one, can then be modified to achieve plyometric drills and combined movement. But this is a process that would take months, and there is no rush to get to it, as I want you to be safe throughout the entire journey. Integrating Exercise into Myotherapy Treatment At Melbourne Massage and Treatment, I incorporate […]

Nov
A meniscus is a cushion type of structure that sits between the femur head and the tibia, on the medial side of the knee and the femur and the fibula on the lateral side of the knee. Its role is to protect any friction between the femur head and the other bonds. In sports activities where there is a lot of stop-and-go or stop-and-twist type of motion, such as basketball or netball, the meniscus is put under intense stress, and the chance of injuries can increase. Meniscus tear classification? A meniscus tear is a type of injury that can be classified based on its severity and size. There are different types of classifications, but the most used and accepted is Laprade’s classification (LaPrade et al., 2014). Laprade classification of Meniscus root tears (MRTs) is based on the morphology during arthroscopic assessment. The classification includes five distinct lesions: Type 1 tears represent partial root tears that are stable (7% of all meniscus root tears). Type 2 tears represent complete radial tears within 9 mm of the root attachment centre (67.6%). This type of tear is then subdivided in three other sub-group based on the distance of the tear from the center of the root attachment (2A 0–3 mm, 2B 3–6 mm and 2C 6–9 mm). Type 3 tear was defined as bucket-handle tear with complete root detachment (5.6%). Type 4 tears are complex oblique tears with complete root detachment (10%) and bony avulsion of the root attachment (9.9%). Meniscus tear symptoms In order to diagnose a meniscus tear, the gold standard method is an MRI scan. That said, nowadays, the only time you would get an MRI scan to your knee for a meniscus injury, is for surgery purposes, as we now know, that live with a meniscus tear is possible, as long as the muscle that across the knee joint are well looked after. That said, in the early stage, the symptoms of meniscus tear can include: Joint swelling Tenderness in the knee on the medial or lateral portion of the knee A feeling of catch in the knee as is moving Limited range of motion A feeling of the knee not able to hold the weight. Localised pain To alleviate the discomfort, the aid of a crutch, especially in the early stage, is recommended, and as per all acute phase injuries, the first few days, rest and movement with pain-free range of motion are extremely important. In addition to this, heat can be applied for intervals of 15 minutes once or twice a day. How do we rehabilitate a meniscus tear? As with all injuries, there is not one rehabilitation process that works for everyone, but there are guidelines that can be used to lead a recovery process. Let’s start with the acute phase (first phase), which is the first 72 hours. In this time frame, we would avoid putting direct weight on the affected side and, where possible, do simple knee flex/ext pain-free movements. Placing a pillow under the knee could help avoid locking the knee, which may not feel comfortable. Second phase: In this phase, which would be somewhere after the initial 72 hours, if it feels comfortable, we can start placing some gentle weight on the knee, even though using a crutch can still be acceptable, especially in the early stage of this phase. The second phase can last up to 5 or 6 weeks. An active range of motion, where the knee flexion is always greater, and the knee extension is getting closer to full extension, would keep increasing daily. In this phase, we can introduce Isometric exercises for knee flexion and extension. Those types of exercises can be done with a bench curl machine or an elastic band or ankle weight. What is most important is to start with lightweight or resistance, hold the weight for 40 seconds, and release for 40 seconds. The time frame can be adapted to the patient’s comfort. Halfway through this phase, we can start to introduce eccentric and concentric loads with weights and potential assisted sit and stands type of movement, with a chair that is higher than average and something in front of the patient where they can hold on to (like the back of another chair). As the patients’ confidence and muscles start responding more and more to these exercises, we can move to the third phase, and here we are in week 7 or 8. The chair for sitting and standing is now at average height; we may not need anterior assistance anymore. It is now essential to ensure the patient is walking and confident about placing weight on the affected side. Single-leg squats can be initiated, maybe even with the aid of a stick initially, and day by day without. The load on the anterior and posterior chain muscles of the thigh is increased, and as we move forward from week 10 to week 12, plyometric exercises can be introduced. Along those exercises, we look into explosive lunge, squatting, skipping the rope and running. A great test would be the hopping test, which consists of single-leg hopping, side to side. One minute of oping should not reproduce any pain. All these progressions are approximations of a natural healing process, and based on the individual presentation, this protocol can be modified and enriched as needed. Meniscus tear and surgery. In their meta-analysis of 6 randomised control trials, Meng et al., 2024, concluded that data favor exercise therapy over surgery as a first intervention for meniscus tears. These conclusions come from the fact that the pain reduction, estimated with the knee Knee Injury and Osteoarthritis Outcome Score (KOOS), does not show any difference between the arthroscopic partial meniscectomy (APM) and exercise therapy. That said, it doesn’t mean that surgery is never an option. What Meng et al., 2024 prove is that before heading for an invasive procedure, it is worth it to look into exercise therapy on its own. If the conservative method does […]
Oct
At Melbourne Massage and Treatment in Coburg, we frequently encounter clients dealing with tennis elbow (lateral epicondylitis) and golfer’s elbow (medial epicondylitis). These conditions can cause significant discomfort and limit your ability to enjoy sports and everyday activities. While they are often associated with repetitive arm and wrist movements, it’s essential to consider how poor shoulder mobility and stability can contribute to these issues. What Are Tennis and Golfer’s Elbow? Tennis Elbow Tennis elbow affects the outer part of the elbow, causing pain and tenderness on the outside. This condition typically arises from overuse of the forearm muscles, especially those responsible for wrist extension. Activities such as painting, or even prolonged computer use, or overstreching of extensor muscles can trigger this condition. Golfer’s Elbow Conversely, a golfer’s elbow affects the inner part of the elbow, leading to pain on the inside. This condition is commonly associated with activities that require gripping, flexing the wrist, or repetitive forearm movements, such as golfing, throwing, or lifting. In this presentation is the common flexor tendon that get’s irritated, and refer with pain. The Connection to Shoulder Mobility and Stability While tennis and golfer’s elbow are localized conditions, they often stem from dysfunctions higher up in the kinetic chain, particularly in the shoulder. Poor shoulder mobility and stability can lead to compensatory patterns that place undue stress on the forearm and elbow joints. Shoulder Mobility Limited shoulder mobility can restrict the natural range of motion for various activities. For instance, if your shoulders lack mobility, you may overcompensate with your forearm muscles during tasks that require reaching, lifting, or throwing. This overcompensation can lead to strain, resulting in conditions like tennis or golfer’s elbow. To maintain proper shoulder mobility, you want to ensure the use of the glenohumeral joint along your exercises and move it with specific drills, as this would stimulate the joint synovial fluid and maintain the joint lubricated. On the other hand, if the joint is hypermobile, we should look into how to stabilize it better. Shoulder Stability Shoulder stability is crucial for maintaining proper alignment during movement. Weakness in the shoulder stabilizers can cause the shoulder joint to become unstable, leading to altered movement patterns. When the shoulder isn’t stable, the body often compensates by engaging the forearm and elbow excessively, increasing the risk of injury. As mentioned in the paragraph above, this is what would occur when someone presents with a hypermobility body. In the hypermobility presentation, the ligaments are more lax and don’t hold back the joint movement as expected. Assessing and Addressing the Issue At Melbourne Massage and Treatment, we recommend a comprehensive approach to address tennis and golfer’s elbow effectively: Assessment of elbow epicondylitis Understanding the root cause of your pain is vital. During an initial consultation, we still mainly focused on your elbow presentation and addressed what movement reproduced the discomfort. But not only that. Throughout a tailored investigation, we will address what could be the root cause of the problem. This way, it would be easier to develop a tailored treatment plan. Treatment for elbow epicondylitis Massage Therapy: Targeted massage can alleviate tension in the forearm and improve blood flow, promoting healing. MDN: Myofascial Dry Needling plays a really effective role in tendinitis management. It focuses on targeting the underactive muscles, restoring the neural connection between the central nervous system and muscle, and desensitizing the painful area. Mobilisation: Mobilisation is an ideal technique to address mobility issue, and improve the range of motion of a joint. For epicondylitis presentations, the mobilisation could focus on wrist, elbow or shoulder. This would be based on the finding along the assessment. Strengthening Exercises: In the exercise program, we will initially focus on exercises that can desitentize the elbow area, such as isometric holds, and then move to eccentric and concentric exercises. In this second step, we would already focus on specific shoulder mobility or stability exercises, as needed. Education Understanding proper biomechanics can empower you to make lifestyle changes that prevent future injuries. Giovanni will guide you through exercises and techniques to maintain shoulder health and prevent elbow pain. Conclusion Tennis and golfer’s elbow can be debilitating, but addressing shoulder mobility and stability is key to recovery and prevention. At Melbourne Massage and Treatment in Coburg, Giovanni is dedicated to helping you achieve optimal function and well-being. If you’re experiencing symptoms of tennis or golfer’s elbow, don’t hesitate to contact Giovanni or Book Now your 15-minute free phone consultation to learn more about a personalized assessment and treatment plan. Together, we can work towards getting you back to the activities you love, pain-free. FAQ Q: What are tennis elbow and golfer’s elbow? A: Lateral epicondylitis, affects the outer part of the elbow, causing pain due to overuse of the forearm muscles, particularly those responsible for wrist extension. Common activities that can trigger it include painting and prolonged computer use. Medial epicondylitis, impacts the inner part of the elbow, leading to pain often associated with gripping, flexing the wrist, or repetitive movements like golfing or throwing. Q: How are shoulder mobility and stability related to these conditions? A: Poor shoulder mobility can lead to overcompensation by the forearm muscles during activities requiring reaching, lifting, or throwing. Similarly, weak shoulder stabilizers can cause the shoulder joint to become unstable, forcing the forearm and elbow to work harder, which increases the risk of injury. Both factors contribute to the development of tennis and golfer’s elbow. Q: What are the signs of limited shoulder mobility? A: Signs include restricted movement during overhead activities, difficulty reaching behind your back, and discomfort during routine tasks that involve lifting or throwing. These limitations can lead to compensatory movements that stress the elbow. Q: How do you assess tennis or golfer’s elbow at Melbourne Massage and Treatment? A: We conduct a thorough assessment that focuses on your elbow presentation, identifying movements that reproduce discomfort. This investigation also explores potential underlying issues related to shoulder mobility and stability, helping us understand the root cause of […]
Sep
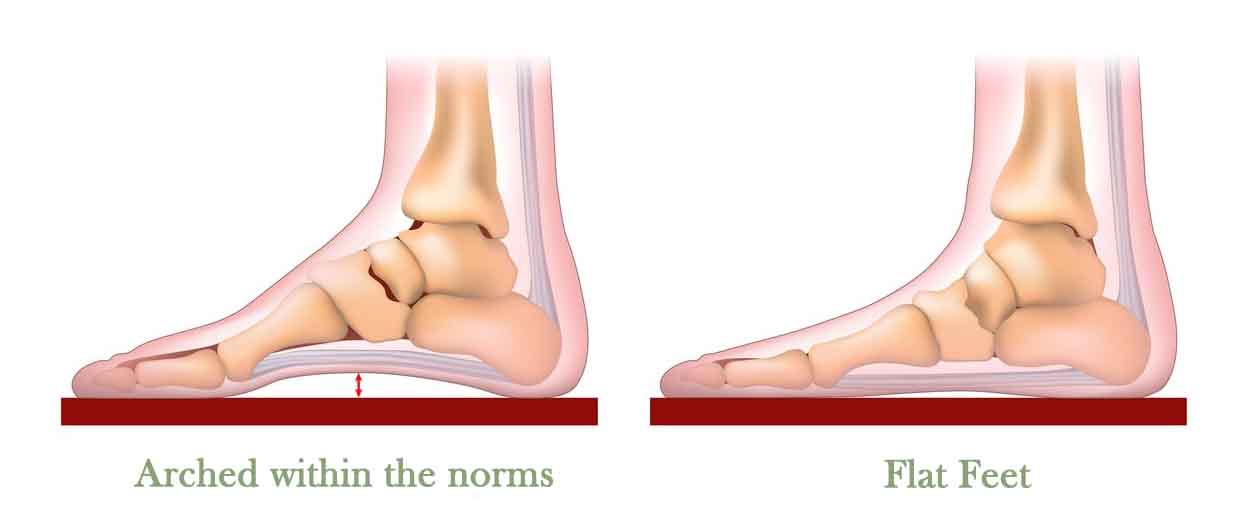
Fallen arches, or Flat Feet, are often misunderstood and can be a source of concern for many. However, as a Clinical Myotherapist, I want to reassure you that flat feet are not inherently problematic. In fact, they can be pretty standard and, in many cases, don’t require any treatment at all. Let’s learn why. Understanding Flat Feet (FF) When the feet’ arch presents as flat, what is occurring is a flat foot, resulting in the entire sole of the foot making contact with the ground. What you may not have noticed yet is that this presentation can be triggered by being on your feet, as in standing on it, and not by lying down or in a seated position with the feet off the ground. This is what we would call structural FF. What are Structural Flat Feet? Structural FF also known as rigid FF , involve an anatomical abnormality where the arch does not form properly. This “malformation” could be caused by genetic factors or developmental issues. What the arch would look like is lower than usual or absent entirely, which is often a lifelong condition. Now, despite their appearance, structurally flat feet are less likely to lead to pain or discomfort. The body, indeed, as it is a functional bio-machine, would easily adapt well to this anatomical variation, and many people with structural flat feet can lead active and healthy lives without any special interventions. Different is the anatomical presentation for functional flat feet, and let’s see why. Functional Flat Feet Functional FF on the other hand, result from how the foot functions rather than an inherent structural issue. In this case, the foot arch may appear flat when standing or walking due to excessive strain or an imbalance in the muscles and tendons that support the arch. When the foot is not bearing weight, the arch may appear normal. Potentially, you could also have one flat foot and one that isn’t when having a functional presentation. This is a common one for those who suffer from structural scoliosis. The main reasons why you may present with functional FF is due to muscle Imbalance, within the foot and ankle. This might be due to overuse, poor posture, or repetitive stress. Other reasons include conditions such as overpronation or excessive weight. Addressing these underlying issues can often alleviate the problem. What can be done for Functional Flat Feet? Changing in foot wear, could be an option. Based on the activity that you are doing on a daily basis life, certain types of footwear may help more than others. Orthotics, which are custom or over-the-counter arch supports, can provide temporary relief and improve function, but these often are over-estimated tools that get prescribed at random. Exercises: Strengthening exercises for the feet and lower legs can help improve muscle balance and support the arch, reduce the pain and improve motor function. In some cases, as explained in this study by Sanchez-Rodriguez et al. (2020), exercises can change the shape of the feet for the better if the intervention is done at an early age; in others, it can help maintain the feet pain-free. When Should You Worry? Most people with flat feet experience no symptoms, and if that’s the case, you do not need to worry about changing the presentation, as it could lead to pain and discomfort. If you are experiencing pain, on the other hand, is worth it to consult an health care practitioner, that can be a podiatrist, or book an appointment at Melbourne Massage and Treatment, where we are going to evaluate if the pain is due to the flat feet it self, or to other conditions such as plantar fasciitis, shin splints, or other pathologies. The Bigger Picture It’s essential to remember that FF are just one of many variations of normal foot anatomy. They do not necessarily indicate a health problem or affect your overall well-being. For most individuals, flat feet are simply a characteristic of their body and do not require any special treatment. In conclusion, whether you have structural or functional flat feet, it’s essential to focus on how you feel and function rather than the appearance of your feet. In many cases, flat feet are perfectly normal and do not pose any significant health risks.
- 1
- 2