
A pain response is a signal created by the brain to let you know that something within the body is not right, or at least, that something, potentially, is not right. This means that pain is a sensation that can also be there when no actual damage is present in the first place. But when you feel pain in the neck, in the shoulder, in the knee or somewhere, how can you differentiate if it is a pain given by muscles or by a joint? In this blog, I want to talk about the difference between muscle pain and joint pain. Muscle and Joint Pain: Let’s Start With Clinical History Intake When someone presents to the clinic in pain, the first thing I do is to track down their medical history, which includes their daily activities, previous injuries (old and recent), sports history, medications, quality of sleep, etc.. From there, I start to narrow down when they have been experiencing the pain, and what caused it in the first place, and where they feel it. Already, that information can give a good perspective of what we are looking at, in terms of muscle pain and joint pain. Knowing the time frame of the pain, the location of the pain can already give an answer. But before jumping to conclusions, we need to do some testing Active and Passive Movement: The Differences In Pain Response After an accurate intake of the clinical history, we would proceed with some testing, including active and passive range of motions. Active range of motions (AROM) are those movements that the patient would do on their own, like flexing the shoulder, rotating the hip, etc Passive range of motions (PROM), on the other hand, are movements that the therapist would do with the patient’s body. So you will be asked to keep your arm and shoulder relaxed, and it will be the therapist who moves the arm. Here is where things start to get interesting. If you respond with pain with AROM, we know that you are using both your muscle and joint to deliver the movement, so the pain response that you feel could be either from the muscle or the joint. But if you respond with pain with a PROM, then we know that the response is from the joint, because the muscle, in that specific motion, is not working. How about tendon? So, when delivering a PROM, we may push the movement to its limit, creating a stretch motion. This specific endpoint of movement, if it reproduces a really pinpoint specific pain, that is sitting right on to what we can recall as a tendon (the insertion point of the muscle), it is another differential tool to understand what the pain is caused by. So yes, to simplify, we use PROM to identify a joint pain, but in that joint pain, we include the tendon itself, not only the ligaments. Ligaments, per clarification, are the tissues that hold the bones together and make up the joint. Orthopedic testing: another tool for differentiating muscle pain from joint pain But the rabbit hole of understanding where that pain is from doesn’t stop here. That’s why we also use orthopedic testing when looking at a pain presentation. Ortopedic testing is a test that places stress on a specific structure, and can have a range of sensitivity and specificity. Sensitivity refers to the test’s ability to identify individuals who have the condition being tested for. Specificity refers to its ability to identify individuals who do not have the condition. Those two terms, that get evaluated in %, can tell us how valuable a test is. And most often, to validate a hypothesis of what can cause the pain, we have to use multiple forms of testing, from AROM to PROM to orthopedic testing and Clinical History. Neck Pain: Muscle Pain or Joint Pain – A case study Neck or upper shoulder pain is one of those common presentations, where the patient presents thinking that it is due to a muscle issue, but then, you prove to them that it is actually their joint that is the issue. Who is Peter, and with what pain does he present himself? Let’s examine a case study of Peter (name of fantasy), a 43-year-old office worker presenting with pain radiating from his right neck to the upper shoulder. Despite various stretches, the pain persists. He tried many pillows, he tried any sleep position, but this pain comes and goes, and has been on for years. Peter presents with a pain level today of 7/10, complaining that certain neck movements are limited and painful. It is hard, for example, to do a head check while driving. Clinical History So, first thing I would do is go through Peter’s clinical history and find out that his pain started about 10 years ago, after a whiplash accident, and that at that time, more than having a collar on his neck for a week or two, he hadn’t done much about it. Hi pain, which occasionally radiates to the neck, also gives him a headache. Sport history includes playing AFL from when he was a kid till his mid-twenties, and nowadays the occasional swim, yoga and pilates class. He spends most of his days working from home or at the office, sitting in a chair. In addition to this, we also know that: No pain radiating down the arms, no pins and needles in the hands; Pain is worst in the morning; Stretching gives an initial relief, but then it gets worse. Differential Diagnoses (DD) Differential diagnoses are the hypotheses we think of when someone presents with pain. Let’s say that is what we think we could find as a problem, given the patient’s complaint we received. And out of 3 or 4 DD’s, we will draw a line that connects all the results and get a Working Diagnosis (WD), which is the most plausible answer given the results we obtained. This said, this […]
Tag Archives: joint pain

Blog
It Is Never Too Late To Join A 1:1 Fitness Class
At Melbourne Massage and Treatment in Fitzroy North, as a clinical Myotherapist, I am enthusiastic [...]
Continue readingMar

Blog
MLD vs Lymphatic Massage: A Clinician’s Guide to What Works and Why
If you’re searching for lymphatic therapy in Fitzroy North, it’s common to see terms like [...]
Continue readingFeb

Blog
Shoulder Pain Isn’t Just a Shoulder Problem
Shoulder pain is one of those presentations that can stop you from enjoying your day. [...]
Continue readingFeb

Blog
Glutes strengthening – Time To Exercises
Here in Fitzroy North, at my Myotherapy Clinic and 1:1 fitness class studio, I get [...]
Continue readingFeb
Blog
Calf Injury Melbourne – How Can Myotherapy Help With Rehab?
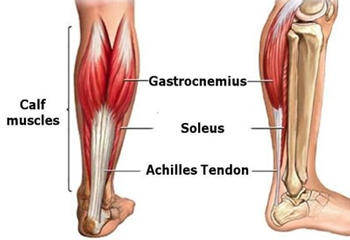
Calf injuries, such as a muscle tear, can be annoying to deal with because they [...]
Continue readingFeb

Aug
Modern life places ongoing pressure on both body and mind, leaving many Australians searching for natural ways to restore calm. Muscle tightness, fatigue, and poor sleep are often signs that stress has taken hold. At Melbourne Massage and Treatment, remedial massage is used as a practical therapy to release tension, regulate the nervous system, and support wellbeing, offering a balanced pathway to sustained relaxation and resilience. Key Takeaways Stress affects both body and mind Remedial massage releases tension and restores balance Circulation and sleep improve with regular sessions The nervous system resets during treatment Melbourne Massage and Treatment offers expert support What is Remedial Massage? Remedial massage is a form of therapeutic massage that targets specific muscles and tissues to relieve pain, promote healing, and improve function. It combines various techniques, including deep tissue work, trigger point therapy, myofascial release, and stretching, to address both acute and chronic conditions. Unlike relaxation massage, which focuses on general relaxation, remedial massage is tailored to treat specific problems in the body, such as muscular tension, joint pain, and postural imbalances. The key difference between remedial and other types of massage is that it aims to treat underlying physical issues and dysfunctions, which can, in turn, help to alleviate the mental and emotional effects of stress. Stress can manifest physically in the body in various ways, including muscle tension, headaches, poor posture, and fatigue. Remedial massage directly addresses these physical symptoms, creating a ripple effect that helps to calm the mind and restore balance. How Remedial Massage Reduces Stress? Stress doesn’t just impact your mind; it can manifest physically in the body, resulting in tight muscles, headaches, neck pain, back discomfort, and other ailments. When the body is under stress, it produces higher levels of cortisol harmone, a hormone linked to the body’s “fight or flight” response. This can lead to increased muscle tension, heart rate, and even digestive issues. Remedial massage works by targeting these physical manifestations of stress and promoting relaxation in several ways. 1. Reduces Muscle Tension One of the most immediate and noticeable benefits of remedial massage is its ability to reduce muscle tension. When we experience stress, we often unconsciously tighten our muscles, especially in areas like the neck, shoulders, back, and jaw. Over time, this chronic muscle tightness can lead to pain, discomfort, and restricted movement. Remedial massage helps to release this built-up tension by applying pressure to specific muscle groups, promoting blood flow, and encouraging the muscles to relax. Targeted Techniques: Techniques such as deep tissue massage and trigger point therapy can focus on areas where muscle tightness tends to accumulate due to stress. These methods help to break up muscle knots and reduce the overall tension in the body. Increased Blood Flow: By improving circulation, remedial massage enhances the delivery of oxygen and nutrients to tissues, promoting healing and relaxation. 2. Activates the Parasympathetic Nervous System The autonomic nervous system consists of two branches: the sympathetic nervous system (SNS), which triggers the ‘fight or flight’ response, and the parasympathetic nervous system (PNS), which manages the ‘rest and digest’ state. Chronic stress keeps the SNS activated, which can leave the body in a constant state of alertness. Remedial massage stimulates the PNS, encouraging the body to relax and return to a state of calm. Relaxation Response: When the PNS is activated, heart rate and blood pressure drop, and the body enters a state of relaxation. This not only helps with muscle relaxation but also reduces anxiety and promotes overall mental well-being. Lowering Cortisol Levels: By activating the PNS, remedial massage helps to lower cortisol levels in the body. This reduction in cortisol can help combat the harmful effects of prolonged stress, such as anxiety, poor sleep, and immune system suppression. 3. Improves Sleep Quality Stress often leads to poor sleep, whether through difficulty falling asleep or waking up throughout the night. One of the ways that remedial massage helps to combat stress is by promoting better sleep. Through its calming effects on the nervous system and muscle relaxation, massage encourages a deeper, more restful sleep. Relaxation Before Bed: A remedial massage session before bed can help you unwind from the day’s stress, allowing you to go to sleep feeling relaxed and at ease. Improved Sleep Cycle: By reducing tension and lowering cortisol levels, remedial massage helps to improve the quality of sleep, leading to more restorative rest and reduced feelings of stress the following day. 4. Reduces Anxiety and Enhances Mood Stress and anxiety often go hand in hand. While stress tends to be a response to external pressures, anxiety can become a persistent feeling that affects your mental health. Remedial massage has been shown to have a positive impact on mental health, particularly by reducing anxiety and boosting mood. Endorphin Release: Massage stimulates the release of endorphins, natural chemicals in the brain that promote feelings of well-being and happiness. This helps to counteract the negative effects of stress and anxiety, providing a natural mood lift. Emotional Release: For some individuals, massage can facilitate an emotional release, allowing pent-up emotions from stress to surface. This can be therapeutic and contribute to a feeling of emotional lightness and mental clarity. 5. Improves Posture and Reduces Pain Chronic stress can lead to poor posture, which, in turn, can contribute to musculoskeletal pain. When we’re stressed, we tend to slouch or hunch over, especially when working at a desk for long periods. This poor posture can lead to discomfort in the back, shoulders, and neck, further exacerbating stress. Remedial massage works by improving posture and reducing musculoskeletal pain. Postural Correction: Remedial massage helps to release tight muscles and realign the body, improving posture and reducing the discomfort associated with poor alignment. Pain Relief: By targeting specific areas of pain, remedial massage can relieve discomfort in muscles, joints, and connective tissue, contributing to an overall sense of well-being. Additional Benefits of Remedial Massage for Stress Relief In addition to the direct effects on the body and mind, remedial massage offers […]

Aug
Thai yoga combines assisted stretching with mindful breathing to restore mobility, release tension, and create deep relaxation. At Melbourne Massage and Treatment, this approach blends traditional techniques with professional care, allowing clients to experience greater freedom of movement and a calmer state of mind. With its unique mix of yoga-inspired postures and therapeutic massage, Thai yoga holistically supports both body and mind. Key Takeaways Thai yoga blends stretching, mobility, and relaxation It improves flexibility and posture Stress relief is a core benefit Sessions are fully guided and accessible to all Melbourne Massage and Treatment tailors each session to your needs What is Thai Yoga? Thai Yoga, also known as Thai yoga massage or Thai bodywork, is a traditional healing practice that originated in Thailand over 2,500 years ago. It combines elements of: Yoga-style stretching Acupressure Mindful breathing Meditative touch Unlike a regular massage or a typical yoga class, Thai Yoga is a partner-based practice. The practitioner gently guides you through yoga-like stretches and poses while applying pressure to specific points along the body’s energy lines, known in Thai tradition as Sen lines. The result is a deeply restorative experience that helps release tension, increase range of motion, and calm the nervous system, all without you having to lift a finger. At Melbourne Massage and Treatment, Thai yoga is offered as part of a tailored approach to mobility, posture, and recovery. Mobility: Loosening Up the Joints and Muscles One of the biggest benefits of Thai Yoga is improved mobility. Many of us deal with tight hips, sore backs, or stiff shoulders, whether from sitting all day, overtraining, or simply getting older. Thai Yoga works to gently open up these areas by: Stretching muscles in a passive and supported way Mobilising joints through guided movement Increasing circulation and blood flow to tight or stagnant areas This kind of assisted stretching helps lengthen muscles and fascia (the connective tissue that surrounds your muscles), which improves flexibility and reduces the risk of injury. And because you’re not doing the work yourself, your body can fully relax into each movement, allowing for a deeper and safer stretch than you might achieve on your own. Relaxation: More Than Just Taking It Easy Sure, we all love a good nap or a lie-down on the couch. But true relaxation goes deeper than just stopping activity, it’s about letting the body and mind fully switch off, so healing and recovery can happen. Thai Yoga encourages this state of deep rest through: Rhythmic, flowing movements that calm the nervous system Mindful breathing to slow the heart rate and promote stillness Gentle compression and touch that creates a sense of grounding and safety After a session, many people report feeling lighter, looser, and mentally clearer. Some describe it as a moving meditation or a “body reset.” If you’ve been feeling strung out, overwhelmed, or physically tight, Thai Yoga might be the reset button you didn’t know you needed. Who Can Benefit from Thai Yoga? Thai Yoga is suitable for a wide range of people, including: Office workers who sit for long hours and need to improve posture and mobility Athletes or gym-goers looking to aid recovery and reduce tightness Older adults want gentle movement and joint support People dealing with stress, anxiety, or sleep issues Anyone wanting to improve flexibility, body awareness, or simply relax The best part? You don’t need any yoga experience. Thai Yoga is fully guided, and each session can be adapted to suit your body, flexibility, and needs on the day. What Happens in a Thai Yoga Session? Here’s what you can expect during a typical Thai Yoga session: You stay fully clothed in comfortable attire (like gym or yoga wear) The session takes place on a mat on the floor, not a massage table The practitioner uses their hands, thumbs, elbows, knees, or feet to stretch, rock, and apply pressure Sessions can last anywhere from 60 to 90 minutes The experience is quiet, meditative, and deeply calming You’ll be gently moved through a series of postures, from seated twists to spinal stretches, hip openers, and shoulder releases, all while lying down and breathing deeply. For those seeking greater depth, advanced thai yoga practices may also be introduced, incorporating more complex stretches, dynamic flows, and breathwork techniques to further enhance mobility and relaxation. Thai Yoga vs. Traditional Yoga: What’s the Difference? While both practices aim to support flexibility, relaxation, and body awareness, the key difference is that Thai Yoga is done to you, not by you. Traditional yoga involves actively moving into and holding poses, while Thai Yoga is a passive, assisted experience. This makes it ideal for people who: Are you new to yoga or struggle with certain movements Are you recovering from an injury or managing chronic conditions? Prefer a more hands-on approach to bodywork and healing In many ways, Thai Yoga bridges the gap between yoga and massage, offering the best of both worlds. Bringing Thai Yoga into Your Life You don’t have to travel to Thailand to reap the benefits. Thai yoga practitioners are available in cities and regional areas across Australia. Many yoga studios, wellness centres, and massage therapists now offer Thai yoga classes as part of their services. If you’re interested in giving it a go, here are some tips: Look for a certified Thai Yoga practitioner with experience and good reviews Wear loose, comfy clothing (like leggings and a tee) Stay hydrated before and after your session Speak up during the session if any movement feels uncomfortable Approach it with an open mind and no expectations, every session is different Conclusion Thai yoga is more than stretching, it is a practice that restores balance, enhances movement, and promotes deep relaxation. Combining mindful breathing with guided mobility creates space for the body to release tension and recover naturally. Ready to experience the benefits for yourself? Contact us today and book a session designed to improve both mobility and relaxation. FAQ

Dec
As previously spoken in another blog post, sitting on the floor and working at the pc would be a better anatomical position than sitting on a chair. Why does sitting on the floor work better than sitting on a chair? Sitting on a chair is uncomfortable, especially in the long term. As a massage therapist, most of my clients are people who have cervical pain or suffer from headaches. Sitting at a desk for hours does more damage than you may realise. So, let’s start with the lower body portion. Staying seated on a chair does direct pressure on the thigh, and by doing so, muscles like the hamstring and gluteus muscles get compressed. By compressing this group of muscles, they get weak and stop functioning as they should. In addition, direct pressure is also applied to the sciatica nerve, the main nerve of the lower body portion. The piriformis often compresses the Sciatica nerve. This muscle runs beneath the Gluteus Max and connects the medial portion of the sacrum to the greater trochanter of the femur. So, the deactivation of those muscles would then manifest itself when we try to walk or, in any case, extend the leg. As the “firing pattern” blog post shows, the hamstring and gluteus max muscles are crucial in leg extension and help prevent lower back pain. This is what happens to the muscle part of the lower body portion. But this is not the only issue the body faces with so many hours sitting on a chair. There is more. So sitting on a chair does limit the body’s movement. The decline of the body’s movement creates a cascade of side effects, including mobility reduction in joints like the Hip, Ankle, Feet, and Thoracic. As all those joints don’t move, there is also a diminish in the proprioception body/brain. Another issue is the compensation of the stability joint over the mobility joint. Indeed, when a mobility joint gets stiff, the stability joint above and below would try to compensate. What’s a common finding pain-wise with sitting on a chair for long hours? The prevalent finding is a sore neck. The sore neck happens as the thoracic stuff up. Indeed the lower cervical portion of the vertebrae, which are stability joints, try to compensate for the thoracic stiffness and, in the long term, would cause neck pain, shoulder pain and headaches. Sitting on the floor can improve mobility. Sitting on the floor can help improve your mobility by allowing you to move your body in many different ways without the need to stand up. That movements are what your body needs as mobility exercises. That movement is your body’s way of improving its posture. Indeed, movement is a crucial component in pain prevention. And this doesn’t happen on a chair. How to switch habits? As for all the habit changes, this has to be gradual and not radical. So, start sitting on the floor for 1 hour a day. Give yourself the time to adapt to the change. Slowly you can incorporate more hours, but not in a row. Maybe one hour in the morning and one in the afternoon. Also, incorporate some standing time to sitting on the chair and floor. Implement change, too, within your training. You are doing something new, and your body needs to adapt. As shown in this clip, start, start implementing a habit of sitting on the floor by doing step-by-step movements: Step 1: Move one leg forward, and bend down the other knee. Step 2: Bring both knees down Step 3: Swing the lower leg to the side (either Lx or Rx) Step 4: Let your body weight go, and sit down Step 5: Now let your lower leg come forward and sit cross-leg. Step 6: Do from step 5 to step 1 in reverse By clicking here, and here you will find the links to a Thai Yoga exercise that can help a lot with improving hip mobility.
Arthritis can be described as the swelling and tenderness of one or more joints. Arthritis symptoms and types Symptoms include: joint pain stiffness reduce Range of Motion (ROM) Major Types: Osteoarthritis Rheumatoid-Arthritis Said so, Arthritis can be a consequence of another type of disease, like: Ankylosing spondylitis Gout Juvenile idiopathic Psoriatic A. Reactive A. Septic A. Thumb A. Those types of Arthritis manifest in different body areas and can display simultaneously. Symptoms can worsen with the ageing process. What is Osteoarthritis, and what causes it? We refer to osteoarthritis when the cartilage between the bonds that form a joint does wear out. Cartilage is a hard, slippery tissue that sits between 2 bonds, like the knee cap and femur, or between the bond of your fingers and toes. When this protective layer that keeps the two bonds separate does work out, the joint starts swelling due to an inflammatory process, and pain is consequently reproduced. The cause can be joint overloading due to chronic injuries or imbalance within the musculoskeletal system. For example, wearing high heels, or having a high foot arch, can lead to wear in the cartilage of the big toes. There is no cure for this type of arthritis, and pain management, through manual therapy and or medications is what so far can be done. What is Rheumatoid Arthritis, and what causes it? Rheumatoid A. is a disease type where the immune system attacks the joints. For rheumatoid arthritis, there are fewer known reasons why it can happen, but there are some factors that can play a role, such as: Family history Gender Obesity Joint injury Age Diagnoses To diagnose arthritis, you would have to see your GP and go for further investigations such as an X-ray, blood test or other medical investigations process. Massage and Treatment for Arthritis. For this type of condition, massage can be a useful therapeutic tool to reduce the pain sensation and manage the presentation. No massage technique can cure the presentation itself, but techniques like MLD are probably the most effective in pain management and symptom relief. Thanks to the direct stimulation of the Lymphatic System, MLD can inhibit the pain signal and relieve the person. As arthritis is often present in older people, we must check for any other condition or presentation that is an absolute contraindication to this type of treatment before commencing treatment. If this post is talking to you, and you need a massage, book your next session by clicking here.
Apr
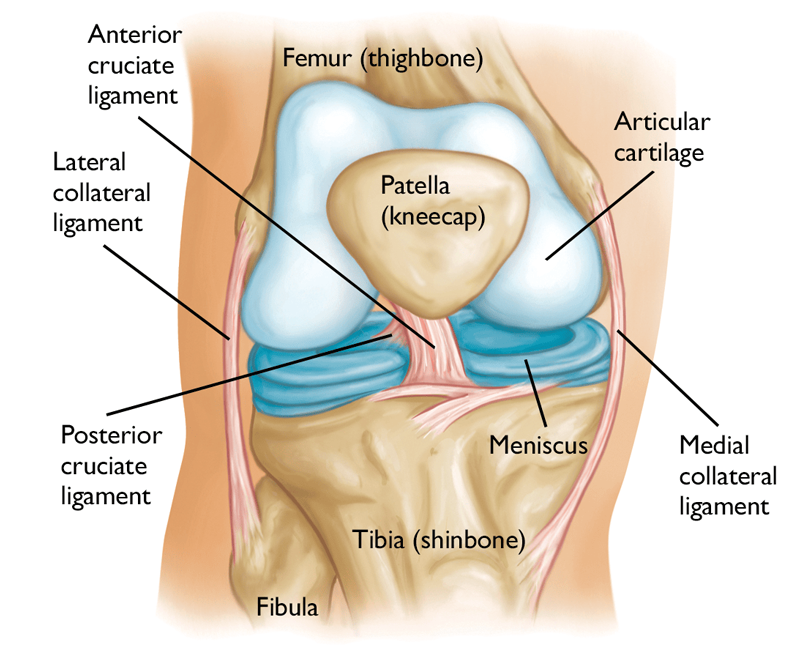
Knee pain is a common presentation for clients of any range of age and gender. Knee pain indeed is a vast topic. So in this post, we are going to go through how to identify the reason why we can experience knee pain. For doing so we are going to look at some special testing, that we use for the knee joints. Next, in a further post, we may analyse individual conditions. What about the Knee Joint? The knee is the strongest joint in the body. It takes a lot of pressure from the upper body and still has to handle the shock coming from the lower leg session, shock as walking, running and jumping. Indeed, whenever we do one of these actions, the knee plays a big role. Knee Anatomy Bond: Above: Femur Below: Medially the Tibia, laterally the Fibula. Patellar is the front “floating bond” Ligaments: Anterior Crucial Ligament Posterior Crucial Ligament Posterior Menisco-Femoral Ligament Fibular Collateral Ligament Tibial Collateral Ligament Transverse Ligament (this one is visible only from the front side of the knee, below the patella). In between the bonds we have: Medial Meniscus Lateral Meniscus If this post is talking to you, book your next massage session by clicking here. So, the knee joint can be divided into two parts: Tibiofemoral joint Connects through the collateral ligaments, cruciate ligaments and menisci; Patellofemoral joint Gives stability to the medial and lateral retinaculum and allows the extension mechanism through the tendons of the quadriceps f.. Now that we have a better idea of what the knee anatomy is, we can look into his functionality. Knee ROM are: Extension: 0° Flexion: 140° Internal Rotation: 30° External Rotation: 40° Abduction/Adduction: 15° Said so, we can see that the major movement that the knee can accomplish is, flexion. Even if the Internal and External rotation since to be a big move for the knee, in the reality, that’s not always the case. The older we get, easily this motion actively gets tighter. Indeed, one of the main reason for meniscus injury is the twisting of the knee, when the feet is holding the ground and the body rotates. But as previously mentioned in this post we would look into the knee special test. What knee functional test have to tell us? As we already mentioned in another post, a generic active, passive or resisted ROM tell us about muscle functionality. On the other hand, a special test for the knee can show us if a ligament or a meniscus is loose, in the case of ligament or injured. Furthermore, special tests, on the knee are essential to prevent further injury and reduce joint degeneration. To start with we have the drawer test: Anterior Draw test and Posterior Draw test. The Anterior one is to test the anterior crucial ligament, and the posterior, obviously, is for the crucial posterior ligament. Both these tests are done with the client lying supine on the table, with a hip and knee flexed, and foot on the table. The therapist will ensure that the foot doesn’t move and will place its hands around the knee, with the fingers (except the thumb) seating at the top of the calf and the thumbs seating on the patella. For the A.D. test, the therapist will lightly pull the knee joint away from the patient body. On the other hand, for the P.D. test, the therapist will push the knee towards the patient’s body. These tests are positive if there is a loose movement within the knee, in the direction of pull or push. If the client has a history of injuries, to the ACL or PCL the therapist wants to make sure not to push or pull with great effort, or injury could occur. Vagus and varus test. Those tests analyse the status of the medial and lateral ligaments. For the valgus test, the therapist places one hand above the knee laterally, and the other hand above the ankle on the medial side. By applying opposite pressure in the 2 directions we put the medial ligament under stress. If pain is reproduced, or there is a loose movement the test is positive. The same action is for the Varus test. In this case, the hands are placed still above the knee and ankle, but the bottom hand is placed laterally and the top one, is placed medially. Apleys Test This test is used to evaluate the state of the meniscus. The client, in this case, would be lying in a prone position, with the knee flexed. The therapist will be standing next to the client, on the side of the knee flexed and will apply pressure to the knee. If no pain is reproduced with pressure only, the therapist can gently apply a rotation movement to the flexed knee. The test is positive if the pain is reproduced. McMurray test. This is luckily the most efficient and most used knee test used by therapists in case of meniscus injury Here is how it works: The patient lies in the supine position with the knee completely flexed (heel to glute). Lateral Meniscus: the examiner then medially rotates the tibia and extends the knee. Medial Meniscus: the examiner then laterally rotates the tibia and extends the knee. McMurray is a positive test if the pain is reproduced. There are still a couple of tests that can be done for the knee, but so far we did cover the most important. About the therapy that I can offer for releasing knee pain, MLD is what I would suggest the most. Especially for acute pain and swelling or oedema reduction. Whereas, Myotherapy or Remedial Massage and Thai Massage can be used too but more to facilitate and or strengthen the muscle surrounding the area.