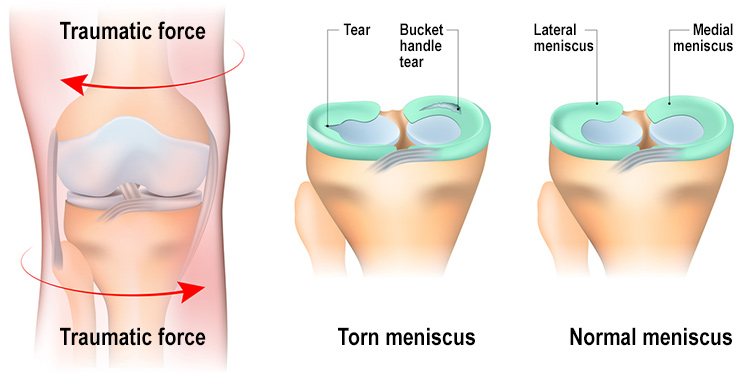
A meniscus is a cushion type of structure that sits between the femur head and the tibia, on the medial side of the knee and the femur and the fibula on the lateral side of the knee. Its role is to protect any friction between the femur head and the other bonds. In sports activities where there is a lot of stop-and-go or stop-and-twist type of motion, such as basketball or netball, the meniscus is put under intense stress, and the chance of injuries can increase.
Meniscus tear classification?
A meniscus tear is a type of injury that can be classified based on its severity and size.
There are different types of classifications, but the most used and accepted is Laprade’s classification (LaPrade et al., 2014). Laprade classification of Meniscus root tears (MRTs) is based on the morphology during arthroscopic assessment. The classification includes five distinct lesions: 
- Type 1 tears represent partial root tears that are stable (7% of all meniscus root tears).
- Type 2 tears represent complete radial tears within 9 mm of the root attachment centre (67.6%). This type of tear is then subdivided in three other sub-group based on the distance of the tear from the center of the root attachment (2A 0–3 mm, 2B 3–6 mm and 2C 6–9 mm).
- Type 3 tear was defined as bucket-handle tear with complete root detachment (5.6%).
- Type 4 tears are complex oblique tears with complete root detachment (10%) and bony avulsion of the root attachment (9.9%).
Meniscus tear symptoms
In order to diagnose a meniscus tear, the gold standard method is an MRI scan. That said, nowadays, the only time you would get an MRI scan to your knee for a meniscus injury, is for surgery purposes, as we now know, that live with a meniscus tear is possible, as long as the muscle that across the knee joint are well looked after. That said, in the early stage, the symptoms of meniscus tear can include:
- Joint swelling
- Tenderness in the knee on the medial or lateral portion of the knee
- A feeling of catch in the knee as is moving
- Limited range of motion
- A feeling of the knee not able to hold the weight.
- Localised pain
To alleviate the discomfort, the aid of a crutch, especially in the early stage, is recommended, and as per all acute phase injuries, the first few days, rest and movement with pain-free range of motion are extremely important. In addition to this, heat can be applied for intervals of 15 minutes once or twice a day.
How do we rehabilitate a meniscus tear?
As with all injuries, there is not one rehabilitation process that works for everyone, but there are guidelines that can be used to lead a recovery process.
Let’s start with the acute phase (first phase), which is the first 72 hours. In this time frame, we would avoid putting direct weight on the affected side and, where possible, do simple knee flex/ext pain-free movements. Placing a pillow under the knee could help avoid locking the knee, which may not feel comfortable.
Second phase:
In this phase, which would be somewhere after the initial 72 hours, if it feels comfortable, we can start placing some gentle weight on the knee, even though using a crutch can still be acceptable, especially in the early stage of this phase. The second phase can last up to 5 or 6 weeks. An active range of motion, where the knee flexion is always greater, and the knee extension is getting closer to full extension, would keep increasing daily. In this phase, we can introduce Isometric exercises for knee flexion and extension.
Those types of exercises can be done with a bench curl machine or an elastic band or ankle weight. What is most important is to start with lightweight or resistance, hold the weight for 40 seconds, and release for 40 seconds. The time frame can be adapted to the patient’s comfort. Halfway through this phase, we can start to introduce eccentric and concentric loads with weights and potential assisted sit and stands type of movement, with a chair that is higher than average and something in front of the patient where they can hold on to (like the back of another chair).
As the patients’ confidence and muscles start responding more and more to these exercises, we can move to the third phase, and here we are in week 7 or 8.
The chair for sitting and standing is now at average height; we may not need anterior assistance anymore. It is now essential to ensure the patient is walking and confident about placing weight on the affected side. Single-leg squats can be initiated, maybe even with the aid of a stick initially, and day by day without. The load on the anterior and posterior chain muscles of the thigh is increased, and as we move forward from week 10 to week 12, plyometric exercises can be introduced. Along those exercises, we look into explosive lunge, squatting, skipping the rope and running.
A great test would be the hopping test, which consists of single-leg hopping, side to side. One minute of oping should not reproduce any pain.
All these progressions are approximations of a natural healing process, and based on the individual presentation, this protocol can be modified and enriched as needed.
Meniscus tear and surgery.
In their meta-analysis of 6 randomised control trials, Meng et al., 2024, concluded that data favor exercise therapy over surgery as a first intervention for meniscus tears. These conclusions come from the fact that the pain reduction, estimated with the knee Knee Injury and Osteoarthritis Outcome Score (KOOS), does not show any difference between the arthroscopic partial meniscectomy (APM) and exercise therapy.
That said, it doesn’t mean that surgery is never an option. What Meng et al., 2024 prove is that before heading for an invasive procedure, it is worth it to look into exercise therapy on its own. If the conservative method does not lead to any positive outcome, surgery could be an option to consider down the line. All of these factors also consider the patient’s disability index and age.
What’s the role of Myotherapy, then?
At Melbourne Massage and Treatment in Fitzroy North, Giovanni offers Myotherapy services for meniscus tear rehabilitation. This type of presentation indeed can be managed with hands-on treatment and exercise protocols. Along Myotherapy intervention Giovanni can focus on joint mobilisation of the knee, deep tissue treatment and dry needling of muscle that cross over the knee joint (quods and hamstring).
After the hands-on treatment comes the exercise program. For best results, you can also apply for a treatment plan that would give you access to 3 or 5 sessions discounted at 10% to use in 8 weeks. During those sessions, Giovanni would ensure you get access to constant therapy, adjustment of the treatment, if and where needed, and personalised care.
Myotherapy treatments are available for NDIS and HICAPS rebates.
In conclusion, if you are suspicious of suffering from a meniscus tear, book now your initial consultation for a Myotherapy treatment or a free 15-minute treatment plan consultation, to better understand how Giovanni can help you in your recovery process.
FAQ – Meniscus Tear
References:
LaPrade, C. M., James, E. W., Cram, T. R., Feagin, J. A., Engebretsen, L., & LaPrade, R. F. (2014). Meniscal Root Tears. The American Journal of Sports Medicine, 43(2), 363–369. https://doi.org/10.1177/0363546514559684
Meng, J., Tang, H., Xiao, Y., Liu, W., Wu, Y., Xiong, Y., & Gao, S. (2024). Long-term effects of exercise therapy versus arthroscopic partial meniscectomy for degenerative meniscal tear: A meta-analysis of randomized controlled trials. Asian Journal of Surgery, 47(6), 2566–2573. https://doi.org/10.1016/j.asjsur.2024.03.091
Giovanni La Rocca
Giovanni moved to Melbourne, Australia, from Italy in 2008 and became a citizen in 2017. He started studying massage therapy in 2016, then completed a Bachelor of Health Science in Clinical Myotherapy in August 2024. During those years, he also specialised in Thai Massage and Manual Lymphatic Drainage for presentations like Lipoedema and Lymphoedema. Nowadays, he runs his clinic in Fitzroy North, Melbourne, where he integrates movement therapy into his practice to enhance overall well-being. He also values meditation, having completed several Vipassana courses. Committed to continuous learning, he aims to share his expertise in integrated therapies to help others achieve balance and resilience.