
Shoulder pain is one of those presentations that can stop you from enjoying your day. Rolling in bed becomes difficult; carrying shopping or even sitting there and doing nothing can be frustrating. At Melbourne Massage and Treatment, I got to see many clients who complained of shoulder pain for a variety of reasons. Although one thing that is common with those different types of pain is the imbalance in the mobility stability joint chain, especially in people who do physical labour, repetitive overhead work, or intense gym training. Therefore, while many people expect me to focus only on the sore spot in the shoulder, my myotherapy approach is always broader and more thorough. Yes, I treat the shoulder as the primary concern, but effective, long-term relief comes from understanding why your shoulder is overloaded in the first place. That means looking beyond the glenohumeral joint and assessing thoracic mobility, scapular control, and thoraco-scapular stability, which are key components that are often overlooked but critical for shoulder health and to help you fix the shoulder pain. Why Shoulder Pain Often Persists The Shoulder is a joint characterised by a great amount of mobility and not much stability, which puts it at high risk of injury and so pain. When your shoulder hurts, it’s rarely because the shoulder itself is “weak” or “damaged” in isolation. Indeed, to arrive to the pain response, either you had a severe trauma, like a fall on the shoulder or more commonly, the shoulder is compensating for: Poor thoracic spine mobility Weak or poorly coordinated scapular stabilisers Faulty movement patterns under load Repetitive strain from work or training And let’s be clear, we are all different, so two individuals who do the exact same job or sport may end up having different pain and presentation due to basic anatomical differences in the shoulder. That said, here are some common presentations that can lead to shoulder pain: If the thoracic spine doesn’t move well, the shoulder is forced to work harder. If the scapula doesn’t stabilise properly, the ac joint gets overloaded Genetically, the space between bonds (Humerus and Acromioclavicle joint) is narrower than the norm My Clinical Assessment Process For Shoulder Pain When you come to my Myotherapy Clinic in Fitzroy North for shoulder pain, I don’t just ask where it hurts, but I would assess: Thoracic spine mobility (especially rotation and extension) Cervical movement in active and passive motion Scapular positioning and control Shoulder range of motion under load Training or work-related movement demands Previous injuries or recurring pain patterns This is particularly important if you: Work in trades or manual labour Train heavily in the gym or sport Perform repetitive overhead movements Have had recurring or long-term shoulder pain A tailored assessment, such as the above one, allows me to not only pinpoint why the shoulder is in pain and what further investigation may be needed to confirm the findings but also address these factors, allowing us to understand the underlying drivers of your pain. The Role of Thoracic Mobility in Shoulder Pain The thoracic spine (mid-back) plays a massive role in how your shoulder functions. This is because the thoracic section of the spine is the mobile portion that anticipates the stable scapula-thoracic joint in the mobility, stability chain. Limited thoracic mobility can lead to: Reduced the overhead range Increased strain on the rotator cuff Poor scapular mechanics Neck and shoulder tension As part of the myotherapy treatment protocol for shoulder pain, I often combine manual therapy, joint mobilisation, and movement-based rehab to restore thoracic movement.When the thoracic spine moves better, the shoulder doesn’t have to overwork, pain reduces, and then we can increase the strength by increasing the load. A classic example of the thoracic shoulder relation is a cricket player. The thoracic rotation along the throwing action is essential to optimise the force imprinted during the throwing action. In fact, imagine the thrower in a cricket game, using only the shoulder, and not rotating that thoracic joint chain. The shoulder load would be excessive, and in a short time, it would cause overload injury and so shoulder pain. Scapular Stability: The Missing Link Your scapula (shoulder blade) is the foundation for shoulder movement. Indeed, the scapula-thoracic joint is the stable joint between the thoracic and the glenohumeral mobile joints. But not only that, indeed, the scapula is the origin point of the rotator cuff muscles, a group of muscles that control the positioning of your humeral head in the glenoid fossa. If it lacks stability or control: The shoulder joint becomes vulnerable Tendons are placed under excessive stress Pain persists despite “strengthening” exercises As a Clinical Myotherapist, I focus on improving thoraco-scapular stability, ensuring the shoulder blade moves smoothly and supports the arm during load, lifting, and rotation. This is especially crucial for people involved in: Weightlifting Cross-training Construction or trade work Sports requiring throwing or overhead movement To strengthen the stability of the scapula, we then have to work on the rhomboid muscles and the trapezius (upper, mid, and lower), but even the levator scapulae. So yes, it is not a quick fix to restore shoulder functionality and remove shoulder pain, but there is a step-by-step journey that can be taken, and it is your choice to start walking along this path. I am here only to help you understand what the right path is for your presentation and ensure we take the right route. Hypermobility and Shoulder Pain One often overlooked factor in shoulder pain is hypermobility. Hypermobility means your joints move more than the norms which isn’t always a bad thing, but it significantly increases injury risk when stability is lacking, particularly in the shoulder. For hypermobile individuals: Ligaments provide less passive support Muscles must work harder to stabilise joints Poor scapular stability leads to shoulder overload When hypermobility exists alongside poor thoraco-scapular stability, shoulder pain becomes far more likely. In these cases, treatment isn’t about increasing flexibility; instead would be the opposite: Improving neuromuscular control Enhancing scapular […]
Tag Archives: mobilisation

Blog
Your Neck Matters! 3 Neck Strengthening Exercises To Stop The Pain
Neck pain is such a common presentation, and often I have to hear from my [...]
Continue readingMar
Blog
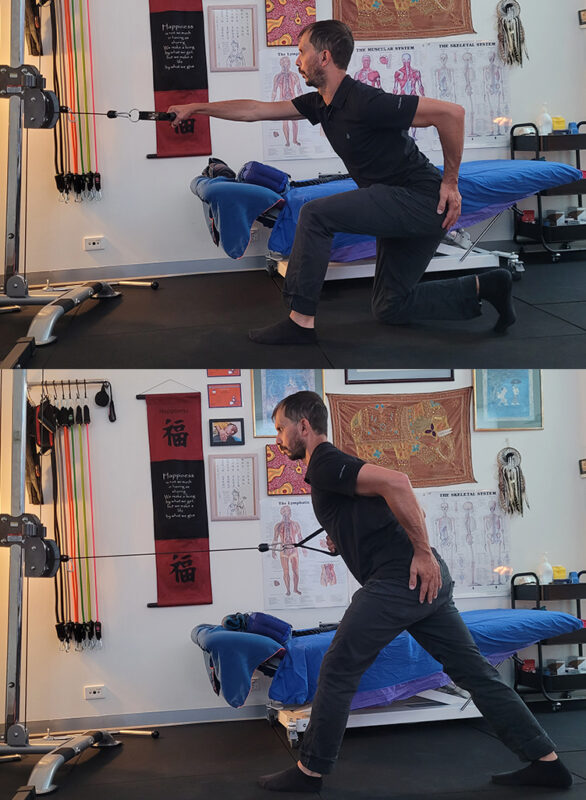
There Is No “Perfect” Lunge. Let’s Find Out Why.
While I guide my client during a 1:1 fitness class at Melbourne Massage and Treatment, [...]
Continue readingMar

Blog
Why the Gluteus Medius Is Essential for Balance, Longevity and Fall Prevention
One thing that can really create terror while we age is falling. No matter the [...]
Continue readingMar

Blog
Chronic Venous Insufficiency and Swollen Legs: Compression Is The Way To Go
In Australia, Chronic Venous Insufficiency (CVI) affect more women than men, with a ratio of [...]
Continue readingMar

Blog
It Is Never Too Late To Join A 1:1 Fitness Class
At Melbourne Massage and Treatment in Fitzroy North, as a clinical Myotherapist, I am enthusiastic [...]
Continue readingMar

Apr
Ankle sprains are among the most common injuries, especially for athletes, active individuals, and even those who simply trip or misstep during daily activities. Despite being a frequent injury, the importance of properly recovering from an ankle sprain is often underestimated. Proper rehabilitation is crucial not only for returning to normal activities but also for preventing long-term complications like chronic instability, arthritis, or re-injury. In this blog, we’ll take a closer look at ankle sprains, their impact on the ligaments involved, and why recovery is so vital for the health of your ankle and the joints above it. What is an Ankle Sprain? An ankle sprain is an injury that occurs to the ankle ligament, which may stretch or be torn. Most commonly, this happens on the lateral portion of the ankle, as the plantar of the feet turn internally. The role of ligaments is to connect bones to each other and provide stability to the joint. In the acute phase of injury, you may experience swelling, pain, bruising, and sometimes instability in the joint. Mechanism of action includes sudden twisting, rolling, or turning motions, like sports or walking on uneven surfaces. Not all ankle sprains are the same, indeed, we have a classification system for it, which is based on their severity: Grade I (Mild): A slight stretching or microscopic tearing of the ligament fibres, typically causing minimal swelling and pain. Grade II (Moderate): Partial tearing of the ligament, with noticeable swelling, bruising, and limited mobility. Grade III (Severe): Complete rupture of the ligament, leading to significant swelling, instability, and difficulty bearing weight. Which Ligaments Are Most Affected? The ankle joint consists of several ligaments, but sprains most commonly affect the lateral (outer) ligaments. These include: The anterior talofibular ligament (ATFL) is the most commonly sprained ligament on the front of the ankle. Calcaneofibular ligament (CFL): A ligament that connects the fibula to the heel bone. Posterior talofibular ligament (PTFL): Less frequently injured, but it can be involved in more severe sprains. Studies show that the ATFL is the most commonly injured ligament, with up to 85% of all lateral ankle sprains involving this ligament (Kerkhoffs et al., 2012). The CFL is also frequently injured, but less commonly than the ATFL. As mentioned above, most often an ankle sprain happens on the lateral portion of the ankle, but in rare cases, the deltoid ligament on the ankle’s medial (inner) side can be sprained, particularly during more forceful or traumatic incidents. Why more laterally than medially? Biomechanically, our ankle finds it easier to turn inwards than outwards. Therefore, it is easier to exceed in ankle inversion (the feet’ plantar face the medial line of the body) than the other way around. This is due to the disposition of the bond in the ankle and feet. The Risks of Not Fully Recovering from an Ankle Sprain Many people recover from an ankle sprain and return to normal activities, but this doesn’t always mean the ankle is fully healed. Incomplete recovery can lead to several risks, including: Chronic Instability: If the ligaments don’t heal properly, the ankle may feel unstable, making it prone to future sprains or injuries. This can create a cycle of repeated sprains, leading to longer-term joint instability. Re-injury: Insufficient rehabilitation increases the risk of re-injury. Returning to physical activity too soon or without proper strength can cause the ligaments to overstretch or tear again. Arthritis: Studies have shown that improper healing of the ankle joint can lead to post-traumatic osteoarthritis (PTOA). This occurs when the joint surfaces are not properly aligned during healing, leading to cartilage degradation over time. Research suggests that 5-20% of individuals who suffer from ankle sprains may develop PTOA later in life (Delco et al., 2017). Muscle Weakness and Atrophy: After a sprain, the muscles around the ankle often weaken due to disuse and immobilisation. This weakness can extend to other areas of the body, increasing the risk of compensatory injuries (e.g., knee or hip strain) as you change how you move to protect the injured ankle. The Benefits of Proper Recovery As with any injury, the recovery process is dictated by your subjective presentation, which includes your clinical history, fitness level, and more. Here are some of the key steps for a full recovery: Achieve strength and joint stabilityThanks to the therapist’s guidance and a mix of treatment and exercises focused on the muscles that cross the ankle joint, like the peroneal and calf muscles, you can regain ankle stability and strength to return to your daily activities. This process can take up to 12 weeks, and its success is based on a mix of your clinical history and effort placed in the recovery process. Reduction in the Risk of Chronic PainPast the acute phase of injury, the risk of developing chronic pain is a common problem for individuals who don’t rehabilitate properly after an ankle sprain. In fact, studies suggest that proper rehab can reduce the risk of long-term pain by improving joint function and reducing stiffness with research indicating that patients who complete a rehabilitation program are 60-70% less likely to experience chronic ankle pain compared to those who don’t (Gribble et al., 2016; Zamperetti et al., 2019). Rehabilitate the Range of MotionA key goal of rehabilitation is to restore the full range of motion (ROM) to the injured joint. Restoring normal ROM is critical for preventing compensatory movements that can strain other joints along the joint chain, like the knee, hip, or lower back. The Recovery Process: What to Expect Proper recovery from an ankle sprain typically involves several stages: Acute Phase (0-72 hours) – P.E.A.C.E: Protect: Safeguard the injured area from further harm and avoid excessive strain. Elevate: Raise the injured area to reduce swelling and improve blood flow. Avoid Anti-inflammatories: Refrain from using anti-inflammatory medications unless advised by a healthcare professional, as they can hinder the natural healing process in some cases. Compress: Apply compression (e.g., with bandages or sleeves) to reduce swelling and provide support. Educate: […]
Oct
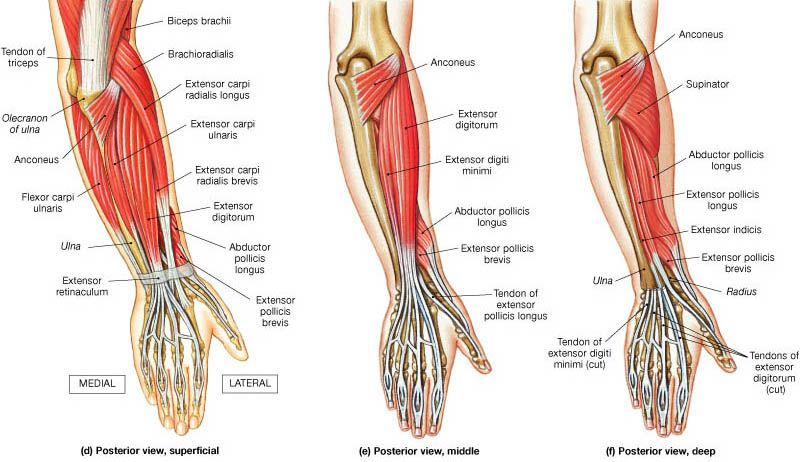
At Melbourne Massage and Treatment in Fitzroy North, we frequently encounter clients dealing with tennis elbow (lateral epicondylitis) and golfer’s elbow (medial epicondylitis). These conditions can cause significant discomfort and limit your ability to enjoy sports and everyday activities. While they are often associated with repetitive arm and wrist movements, it’s essential to consider how poor shoulder mobility and stability can contribute to these issues. What Are Tennis and Golfer’s Elbow? Tennis Elbow Tennis elbow affects the outer part of the elbow, causing pain and tenderness on the outside. This condition typically arises from overuse of the forearm muscles, especially those responsible for wrist extension. Activities such as painting, or even prolonged computer use, or overstreching of extensor muscles can trigger this condition. Golfer’s Elbow Conversely, a golfer’s elbow affects the inner part of the elbow, leading to pain on the inside. This condition is commonly associated with activities that require gripping, flexing the wrist, or repetitive forearm movements, such as golfing, throwing, or lifting. In this presentation is the common flexor tendon that get’s irritated, and refer with pain. The Connection to Shoulder Mobility and Stability While tennis and golfer’s elbow are localized conditions, they often stem from dysfunctions higher up in the kinetic chain, particularly in the shoulder. Poor shoulder mobility and stability can lead to compensatory patterns that place undue stress on the forearm and elbow joints. Shoulder Mobility Limited shoulder mobility can restrict the natural range of motion for various activities. For instance, if your shoulders lack mobility, you may overcompensate with your forearm muscles during tasks that require reaching, lifting, or throwing. This overcompensation can lead to strain, resulting in conditions like tennis or golfer’s elbow. To maintain proper shoulder mobility, you want to ensure the use of the glenohumeral joint along your exercises and move it with specific drills, as this would stimulate the joint synovial fluid and maintain the joint lubricated. On the other hand, if the joint is hypermobile, we should look into how to stabilize it better. Shoulder Stability Shoulder stability is crucial for maintaining proper alignment during movement. Weakness in the shoulder stabilizers can cause the shoulder joint to become unstable, leading to altered movement patterns. When the shoulder isn’t stable, the body often compensates by engaging the forearm and elbow excessively, increasing the risk of injury. As mentioned in the paragraph above, this is what would occur when someone presents with a hypermobility body. In the hypermobility presentation, the ligaments are more lax and don’t hold back the joint movement as expected. Assessing and Addressing the Issue At Melbourne Massage and Treatment, we recommend a comprehensive approach to address tennis and golfer’s elbow effectively: Assessment of elbow epicondylitis Understanding the root cause of your pain is vital. During an initial consultation, we still mainly focused on your elbow presentation and addressed what movement reproduced the discomfort. But not only that. Throughout a tailored investigation, we will address what could be the root cause of the problem. This way, it would be easier to develop a tailored treatment plan. Treatment for elbow epicondylitis Massage Therapy: Targeted massage can alleviate tension in the forearm and improve blood flow, promoting healing. MDN: Myofascial Dry Needling plays a really effective role in tendinitis management. It focuses on targeting the underactive muscles, restoring the neural connection between the central nervous system and muscle, and desensitizing the painful area. Mobilisation: Mobilisation is an ideal technique to address mobility issue, and improve the range of motion of a joint. For epicondylitis presentations, the mobilisation could focus on wrist, elbow or shoulder. This would be based on the finding along the assessment. Strengthening Exercises: In the exercise program, we will initially focus on exercises that can desitentize the elbow area, such as isometric holds, and then move to eccentric and concentric exercises. In this second step, we would already focus on specific shoulder mobility or stability exercises, as needed. Education Understanding proper biomechanics can empower you to make lifestyle changes that prevent future injuries. Giovanni will guide you through exercises and techniques to maintain shoulder health and prevent elbow pain. Conclusion Tennis and golfer’s elbow can be debilitating, but addressing shoulder mobility and stability is key to recovery and prevention. At Melbourne Massage and Treatment in Fitzroy North, Giovanni is dedicated to helping you achieve optimal function and well-being. If you’re experiencing symptoms of tennis or golfer’s elbow, don’t hesitate to contact Giovanni or Book Now your 15-minute free phone consultation to learn more about a personalized assessment and treatment plan. Together, we can work towards getting you back to the activities you love, pain-free. FAQ Q: What are tennis elbow and golfer’s elbow? A: Lateral epicondylitis, affects the outer part of the elbow, causing pain due to overuse of the forearm muscles, particularly those responsible for wrist extension. Common activities that can trigger it include painting and prolonged computer use. Medial epicondylitis, impacts the inner part of the elbow, leading to pain often associated with gripping, flexing the wrist, or repetitive movements like golfing or throwing. Q: How are shoulder mobility and stability related to these conditions? A: Poor shoulder mobility can lead to overcompensation by the forearm muscles during activities requiring reaching, lifting, or throwing. Similarly, weak shoulder stabilizers can cause the shoulder joint to become unstable, forcing the forearm and elbow to work harder, which increases the risk of injury. Both factors contribute to the development of tennis and golfer’s elbow. Q: What are the signs of limited shoulder mobility? A: Signs include restricted movement during overhead activities, difficulty reaching behind your back, and discomfort during routine tasks that involve lifting or throwing. These limitations can lead to compensatory movements that stress the elbow. Q: How do you assess tennis or golfer’s elbow at Melbourne Massage and Treatment? A: We conduct a thorough assessment that focuses on your elbow presentation, identifying movements that reproduce discomfort. This investigation also explores potential underlying issues related to shoulder mobility and stability, helping us understand the root […]

Oct
Joint mobilisations are manual therapy techniques that improve joint mobility and flexibility and reduce joint pain. Joint mobilisation can be applied to many body joints. Some contraindications have to be taken into consideration for mobilisation: Joint swelling Osteo Arthritis Bone Fracture Bulge disk (if the mobs are intended on a vertebra) Mobilisation VS Adjustment. Mobilisations are different from Chiropractic adjustment. The difference is that Chiropractic adjustments are fast movements applied with more significant pressure. Mobilisations are constant slow, repetitive movements applied to the joint. Along with a Myotherapy treatment, Giovanni would evaluate if mobilisation is the proper treatment for your condition. For example, mobilisation along the spine is recommended when someone presents with a stiff back in the sacrum, lumbar, thoracic or lower cervical area. Giovanni would always double-check with you about what the mobs felt like. Types of Mobilisation. As we already know, the body is made of different types of joints. Given the different types of joints, like socket joints, plane joints and more, others are the type of mobilisation. For example: For a joint like the hip, we can apply mobility like a distraction, anterior-to-posterior pressure or posterior-to-anterior pull, internal rotation or superior-to-inferior pull. Some of these techniques can be applied to other joints, and each way of using a mobilisation aims to improve a specific range of motion. So, all up, the type of mobilisation that we have are: Superior to Inferior; Inferior to superior; Distraction; Posterior to Anterior; Anterior to Posterior; Posterior glide; Anterior glide; Lateral glide; Medial glide. Mobilisation Belt. A mobilisation belt can be used to deliver the mobilisation based on the joint we aim to work on. A belt is a tool wrapped around the designated joint we want to work on and is used to apply stretches that would not be as easy to achieve by hand. An example is a hip distraction. For distraction, we refer to it as a force that pulls a joint apart. In the case of a hip, the head of the femur is pulled away from the hip’s socket from the medial to the lateral direction. As you would imagine, using bare hands for applying this technique not only could result in an uncomfortable approach to the intimacy of the patient, but it would requireFr too much effort for the therapist, resulting in poor mobilisation delivery and risk of injury. Therefore, the best tool is a belt wrapped around the patient’s hip and the therapist’s waist. Why use the mobilisation technique? The mobilisation technique aims not to reproduce pain, cracking sound, or sharp sensation. Indeed, the aim is to reproduce a firm pressure/pull on the joint area. Regarding the thoracic area, if any of those vertebrae reproduce pain or sharp sensation, applying the mobs along the vertebrae/ribs joint would be better. Doing so would still possible to affect spine mobility indirectly. Giovanni’s training for this type of modality started during the Advance Diploma in Myotherapy at RMIT and continued at the Bachelor of Health Science at Torrens University. Mobilisations technique can be applied to Big Toe, Ankle, Shoulder, Feet, Hip, Wrist, Elbow, Vertebrae, SIJ joint, Facet Joint, Clavicle and other body areas. An example of joint mobilisation for the feet. Mobilisations at the ankle area are used for improving ankle mobility. Indeed, improving ankle mobility is to better support during the walk, standing and or running. Always talking about the feet area, the mobilisation applied to the Big Toes is used along the Metatasolphalangeal Joint. Do you feel your joints stiff? Your booking for a Myotherapy treatment with Giovanni is just a click away. This mobilisation is applied by creating a distraction movement within the joint, pulling the toes away and then using it for passive flexion and extension. As mentioned in another blog post about wearing bear foot shoes, the Big toes are meant to extend from 65° to 70°. Conclusion The Big Toes are the feet joint that should push the most in the feet strike as we walk. In conclusion, mobilisations are a great way to increase mobility within a joint allowing better movement and improving the range of motion.

Sep
Myotherapy is a massage technique to treat or prevent soft tissue pain and restricted joint movement. “Myotherapy” stands for “Myo” Muscle “Therapy” therapy. In Australia, and specifically in Melbourne, it is a practice that took over the massage market in the last few decades and is not becoming more and more popular. There is Dry Needling and Joint Mobilization along the different techniques used in a Myotherapy treatment. Is Myotherapy Safe? Yes, Myotherapy is a safe treatment. Said so, you want to ensure that the therapist treating you has their qualification up to date. Here is a link to my qualification. What about Dry Needling in a Myotherapy Treatment? Dry needling is one of the many ways a Myotherapist can treat a client, but it is unnecessary. Before using needles, the therapist always has to double-check with the clients the following: No metal allergy No bleeding disorders No needle fear or phobia The client feels comfortable with such treatment The therapist does explain how dry needling works Is Myotherapy available at Melbourne Massage and Treatment? Yes, it is. I am a fully qualified Myotherapist who completed an Advance Diploma in Myotherapy at RMIT University. On top of all, I am now enrolled in the last year of my Bachelor’s Degree in the Myotherapy Clinic at Torrens University. What’s the difference between Myotherapy Treatment and Remedial Massage? Myotherapy is similar to a Remedial Massage session. The difference is that a Myotherapist has more knowledge about the human anatomy, joints, and functionality. So before the session, the therapist would guide the patient through a specific range of motion to evaluate the body’s presentation. Done so, the therapist has an idea of what can be done to improve the body’s presentation. Furthermore, a Myotherapist is trained to use mobilization, which is a repetitive joint movement to improve the joint’s range of motion. My favourite “mobs” are along the spine. They consist of a gentle push over the transverse process of the spine. Applying this constant firm push, the transverse process gain mobility, allowing all the muscle inserts originating from that joint to be more mobile. Is a mobilization the same as what a chiro does? No is not. The Chiro makes an adjustment, which is a fast joint pull or push, to adjust its position or functionality. Along with an adjustment, the patient has no control over the fast movement. Indeed, during mobilisation, the patient can take control of the push and stop the treatment if he/she does feel uncomfortable. Book Now your Myotherapy treatment with Giovanni. Giovanni is available in Fitzroy North at 175 Holden St Monday to Saturday 9 am to 7pm.