
A pain response is a signal created by the brain to let you know that something within the body is not right, or at least, that something, potentially, is not right. This means that pain is a sensation that can also be there when no actual damage is present in the first place. But when you feel pain in the neck, in the shoulder, in the knee or somewhere, how can you differentiate if it is a pain given by muscles or by a joint? In this blog, I want to talk about the difference between muscle pain and joint pain. Muscle and Joint Pain: Let’s Start With Clinical History Intake When someone presents to the clinic in pain, the first thing I do is to track down their medical history, which includes their daily activities, previous injuries (old and recent), sports history, medications, quality of sleep, etc.. From there, I start to narrow down when they have been experiencing the pain, and what caused it in the first place, and where they feel it. Already, that information can give a good perspective of what we are looking at, in terms of muscle pain and joint pain. Knowing the time frame of the pain, the location of the pain can already give an answer. But before jumping to conclusions, we need to do some testing Active and Passive Movement: The Differences In Pain Response After an accurate intake of the clinical history, we would proceed with some testing, including active and passive range of motions. Active range of motions (AROM) are those movements that the patient would do on their own, like flexing the shoulder, rotating the hip, etc Passive range of motions (PROM), on the other hand, are movements that the therapist would do with the patient’s body. So you will be asked to keep your arm and shoulder relaxed, and it will be the therapist who moves the arm. Here is where things start to get interesting. If you respond with pain with AROM, we know that you are using both your muscle and joint to deliver the movement, so the pain response that you feel could be either from the muscle or the joint. But if you respond with pain with a PROM, then we know that the response is from the joint, because the muscle, in that specific motion, is not working. How about tendon? So, when delivering a PROM, we may push the movement to its limit, creating a stretch motion. This specific endpoint of movement, if it reproduces a really pinpoint specific pain, that is sitting right on to what we can recall as a tendon (the insertion point of the muscle), it is another differential tool to understand what the pain is caused by. So yes, to simplify, we use PROM to identify a joint pain, but in that joint pain, we include the tendon itself, not only the ligaments. Ligaments, per clarification, are the tissues that hold the bones together and make up the joint. Orthopedic testing: another tool for differentiating muscle pain from joint pain But the rabbit hole of understanding where that pain is from doesn’t stop here. That’s why we also use orthopedic testing when looking at a pain presentation. Ortopedic testing is a test that places stress on a specific structure, and can have a range of sensitivity and specificity. Sensitivity refers to the test’s ability to identify individuals who have the condition being tested for. Specificity refers to its ability to identify individuals who do not have the condition. Those two terms, that get evaluated in %, can tell us how valuable a test is. And most often, to validate a hypothesis of what can cause the pain, we have to use multiple forms of testing, from AROM to PROM to orthopedic testing and Clinical History. Neck Pain: Muscle Pain or Joint Pain – A case study Neck or upper shoulder pain is one of those common presentations, where the patient presents thinking that it is due to a muscle issue, but then, you prove to them that it is actually their joint that is the issue. Who is Peter, and with what pain does he present himself? Let’s examine a case study of Peter (name of fantasy), a 43-year-old office worker presenting with pain radiating from his right neck to the upper shoulder. Despite various stretches, the pain persists. He tried many pillows, he tried any sleep position, but this pain comes and goes, and has been on for years. Peter presents with a pain level today of 7/10, complaining that certain neck movements are limited and painful. It is hard, for example, to do a head check while driving. Clinical History So, first thing I would do is go through Peter’s clinical history and find out that his pain started about 10 years ago, after a whiplash accident, and that at that time, more than having a collar on his neck for a week or two, he hadn’t done much about it. Hi pain, which occasionally radiates to the neck, also gives him a headache. Sport history includes playing AFL from when he was a kid till his mid-twenties, and nowadays the occasional swim, yoga and pilates class. He spends most of his days working from home or at the office, sitting in a chair. In addition to this, we also know that: No pain radiating down the arms, no pins and needles in the hands; Pain is worst in the morning; Stretching gives an initial relief, but then it gets worse. Differential Diagnoses (DD) Differential diagnoses are the hypotheses we think of when someone presents with pain. Let’s say that is what we think we could find as a problem, given the patient’s complaint we received. And out of 3 or 4 DD’s, we will draw a line that connects all the results and get a Working Diagnosis (WD), which is the most plausible answer given the results we obtained. This said, this […]
Tag Archives: Range of motion

Blog
Your Neck Matters! 3 Neck Strengthening Exercises To Stop The Pain
Neck pain is such a common presentation, and often I have to hear from my [...]
Continue readingMar
Blog
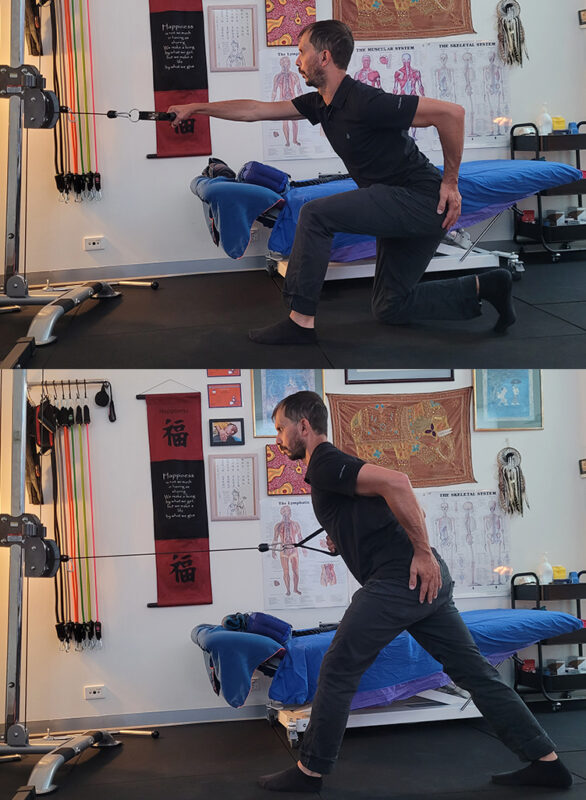
There Is No “Perfect” Lunge. Let’s Find Out Why.
While I guide my client during a 1:1 fitness class at Melbourne Massage and Treatment, [...]
Continue readingMar

Blog
Why the Gluteus Medius Is Essential for Balance, Longevity and Fall Prevention
One thing that can really create terror while we age is falling. No matter the [...]
Continue readingMar

Blog
Chronic Venous Insufficiency and Swollen Legs: Compression Is The Way To Go
In Australia, Chronic Venous Insufficiency (CVI) affect more women than men, with a ratio of [...]
Continue readingMar

Blog
It Is Never Too Late To Join A 1:1 Fitness Class
At Melbourne Massage and Treatment in Fitzroy North, as a clinical Myotherapist, I am enthusiastic [...]
Continue readingMar

Aug
Modern life places ongoing pressure on both body and mind, leaving many Australians searching for natural ways to restore calm. Muscle tightness, fatigue, and poor sleep are often signs that stress has taken hold. At Melbourne Massage and Treatment, remedial massage is used as a practical therapy to release tension, regulate the nervous system, and support wellbeing, offering a balanced pathway to sustained relaxation and resilience. Key Takeaways Stress affects both body and mind Remedial massage releases tension and restores balance Circulation and sleep improve with regular sessions The nervous system resets during treatment Melbourne Massage and Treatment offers expert support What is Remedial Massage? Remedial massage is a form of therapeutic massage that targets specific muscles and tissues to relieve pain, promote healing, and improve function. It combines various techniques, including deep tissue work, trigger point therapy, myofascial release, and stretching, to address both acute and chronic conditions. Unlike relaxation massage, which focuses on general relaxation, remedial massage is tailored to treat specific problems in the body, such as muscular tension, joint pain, and postural imbalances. The key difference between remedial and other types of massage is that it aims to treat underlying physical issues and dysfunctions, which can, in turn, help to alleviate the mental and emotional effects of stress. Stress can manifest physically in the body in various ways, including muscle tension, headaches, poor posture, and fatigue. Remedial massage directly addresses these physical symptoms, creating a ripple effect that helps to calm the mind and restore balance. How Remedial Massage Reduces Stress? Stress doesn’t just impact your mind; it can manifest physically in the body, resulting in tight muscles, headaches, neck pain, back discomfort, and other ailments. When the body is under stress, it produces higher levels of cortisol harmone, a hormone linked to the body’s “fight or flight” response. This can lead to increased muscle tension, heart rate, and even digestive issues. Remedial massage works by targeting these physical manifestations of stress and promoting relaxation in several ways. 1. Reduces Muscle Tension One of the most immediate and noticeable benefits of remedial massage is its ability to reduce muscle tension. When we experience stress, we often unconsciously tighten our muscles, especially in areas like the neck, shoulders, back, and jaw. Over time, this chronic muscle tightness can lead to pain, discomfort, and restricted movement. Remedial massage helps to release this built-up tension by applying pressure to specific muscle groups, promoting blood flow, and encouraging the muscles to relax. Targeted Techniques: Techniques such as deep tissue massage and trigger point therapy can focus on areas where muscle tightness tends to accumulate due to stress. These methods help to break up muscle knots and reduce the overall tension in the body. Increased Blood Flow: By improving circulation, remedial massage enhances the delivery of oxygen and nutrients to tissues, promoting healing and relaxation. 2. Activates the Parasympathetic Nervous System The autonomic nervous system consists of two branches: the sympathetic nervous system (SNS), which triggers the ‘fight or flight’ response, and the parasympathetic nervous system (PNS), which manages the ‘rest and digest’ state. Chronic stress keeps the SNS activated, which can leave the body in a constant state of alertness. Remedial massage stimulates the PNS, encouraging the body to relax and return to a state of calm. Relaxation Response: When the PNS is activated, heart rate and blood pressure drop, and the body enters a state of relaxation. This not only helps with muscle relaxation but also reduces anxiety and promotes overall mental well-being. Lowering Cortisol Levels: By activating the PNS, remedial massage helps to lower cortisol levels in the body. This reduction in cortisol can help combat the harmful effects of prolonged stress, such as anxiety, poor sleep, and immune system suppression. 3. Improves Sleep Quality Stress often leads to poor sleep, whether through difficulty falling asleep or waking up throughout the night. One of the ways that remedial massage helps to combat stress is by promoting better sleep. Through its calming effects on the nervous system and muscle relaxation, massage encourages a deeper, more restful sleep. Relaxation Before Bed: A remedial massage session before bed can help you unwind from the day’s stress, allowing you to go to sleep feeling relaxed and at ease. Improved Sleep Cycle: By reducing tension and lowering cortisol levels, remedial massage helps to improve the quality of sleep, leading to more restorative rest and reduced feelings of stress the following day. 4. Reduces Anxiety and Enhances Mood Stress and anxiety often go hand in hand. While stress tends to be a response to external pressures, anxiety can become a persistent feeling that affects your mental health. Remedial massage has been shown to have a positive impact on mental health, particularly by reducing anxiety and boosting mood. Endorphin Release: Massage stimulates the release of endorphins, natural chemicals in the brain that promote feelings of well-being and happiness. This helps to counteract the negative effects of stress and anxiety, providing a natural mood lift. Emotional Release: For some individuals, massage can facilitate an emotional release, allowing pent-up emotions from stress to surface. This can be therapeutic and contribute to a feeling of emotional lightness and mental clarity. 5. Improves Posture and Reduces Pain Chronic stress can lead to poor posture, which, in turn, can contribute to musculoskeletal pain. When we’re stressed, we tend to slouch or hunch over, especially when working at a desk for long periods. This poor posture can lead to discomfort in the back, shoulders, and neck, further exacerbating stress. Remedial massage works by improving posture and reducing musculoskeletal pain. Postural Correction: Remedial massage helps to release tight muscles and realign the body, improving posture and reducing the discomfort associated with poor alignment. Pain Relief: By targeting specific areas of pain, remedial massage can relieve discomfort in muscles, joints, and connective tissue, contributing to an overall sense of well-being. Additional Benefits of Remedial Massage for Stress Relief In addition to the direct effects on the body and mind, remedial massage offers […]

Aug
Thai yoga combines assisted stretching with mindful breathing to restore mobility, release tension, and create deep relaxation. At Melbourne Massage and Treatment, this approach blends traditional techniques with professional care, allowing clients to experience greater freedom of movement and a calmer state of mind. With its unique mix of yoga-inspired postures and therapeutic massage, Thai yoga holistically supports both body and mind. Key Takeaways Thai yoga blends stretching, mobility, and relaxation It improves flexibility and posture Stress relief is a core benefit Sessions are fully guided and accessible to all Melbourne Massage and Treatment tailors each session to your needs What is Thai Yoga? Thai Yoga, also known as Thai yoga massage or Thai bodywork, is a traditional healing practice that originated in Thailand over 2,500 years ago. It combines elements of: Yoga-style stretching Acupressure Mindful breathing Meditative touch Unlike a regular massage or a typical yoga class, Thai Yoga is a partner-based practice. The practitioner gently guides you through yoga-like stretches and poses while applying pressure to specific points along the body’s energy lines, known in Thai tradition as Sen lines. The result is a deeply restorative experience that helps release tension, increase range of motion, and calm the nervous system, all without you having to lift a finger. At Melbourne Massage and Treatment, Thai yoga is offered as part of a tailored approach to mobility, posture, and recovery. Mobility: Loosening Up the Joints and Muscles One of the biggest benefits of Thai Yoga is improved mobility. Many of us deal with tight hips, sore backs, or stiff shoulders, whether from sitting all day, overtraining, or simply getting older. Thai Yoga works to gently open up these areas by: Stretching muscles in a passive and supported way Mobilising joints through guided movement Increasing circulation and blood flow to tight or stagnant areas This kind of assisted stretching helps lengthen muscles and fascia (the connective tissue that surrounds your muscles), which improves flexibility and reduces the risk of injury. And because you’re not doing the work yourself, your body can fully relax into each movement, allowing for a deeper and safer stretch than you might achieve on your own. Relaxation: More Than Just Taking It Easy Sure, we all love a good nap or a lie-down on the couch. But true relaxation goes deeper than just stopping activity, it’s about letting the body and mind fully switch off, so healing and recovery can happen. Thai Yoga encourages this state of deep rest through: Rhythmic, flowing movements that calm the nervous system Mindful breathing to slow the heart rate and promote stillness Gentle compression and touch that creates a sense of grounding and safety After a session, many people report feeling lighter, looser, and mentally clearer. Some describe it as a moving meditation or a “body reset.” If you’ve been feeling strung out, overwhelmed, or physically tight, Thai Yoga might be the reset button you didn’t know you needed. Who Can Benefit from Thai Yoga? Thai Yoga is suitable for a wide range of people, including: Office workers who sit for long hours and need to improve posture and mobility Athletes or gym-goers looking to aid recovery and reduce tightness Older adults want gentle movement and joint support People dealing with stress, anxiety, or sleep issues Anyone wanting to improve flexibility, body awareness, or simply relax The best part? You don’t need any yoga experience. Thai Yoga is fully guided, and each session can be adapted to suit your body, flexibility, and needs on the day. What Happens in a Thai Yoga Session? Here’s what you can expect during a typical Thai Yoga session: You stay fully clothed in comfortable attire (like gym or yoga wear) The session takes place on a mat on the floor, not a massage table The practitioner uses their hands, thumbs, elbows, knees, or feet to stretch, rock, and apply pressure Sessions can last anywhere from 60 to 90 minutes The experience is quiet, meditative, and deeply calming You’ll be gently moved through a series of postures, from seated twists to spinal stretches, hip openers, and shoulder releases, all while lying down and breathing deeply. For those seeking greater depth, advanced thai yoga practices may also be introduced, incorporating more complex stretches, dynamic flows, and breathwork techniques to further enhance mobility and relaxation. Thai Yoga vs. Traditional Yoga: What’s the Difference? While both practices aim to support flexibility, relaxation, and body awareness, the key difference is that Thai Yoga is done to you, not by you. Traditional yoga involves actively moving into and holding poses, while Thai Yoga is a passive, assisted experience. This makes it ideal for people who: Are you new to yoga or struggle with certain movements Are you recovering from an injury or managing chronic conditions? Prefer a more hands-on approach to bodywork and healing In many ways, Thai Yoga bridges the gap between yoga and massage, offering the best of both worlds. Bringing Thai Yoga into Your Life You don’t have to travel to Thailand to reap the benefits. Thai yoga practitioners are available in cities and regional areas across Australia. Many yoga studios, wellness centres, and massage therapists now offer Thai yoga classes as part of their services. If you’re interested in giving it a go, here are some tips: Look for a certified Thai Yoga practitioner with experience and good reviews Wear loose, comfy clothing (like leggings and a tee) Stay hydrated before and after your session Speak up during the session if any movement feels uncomfortable Approach it with an open mind and no expectations, every session is different Conclusion Thai yoga is more than stretching, it is a practice that restores balance, enhances movement, and promotes deep relaxation. Combining mindful breathing with guided mobility creates space for the body to release tension and recover naturally. Ready to experience the benefits for yourself? Contact us today and book a session designed to improve both mobility and relaxation. FAQ
Oct
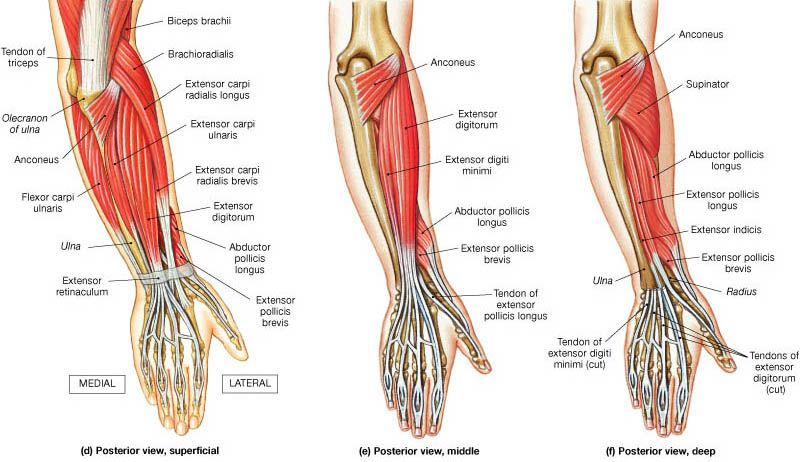
At Melbourne Massage and Treatment in Fitzroy North, we frequently encounter clients dealing with tennis elbow (lateral epicondylitis) and golfer’s elbow (medial epicondylitis). These conditions can cause significant discomfort and limit your ability to enjoy sports and everyday activities. While they are often associated with repetitive arm and wrist movements, it’s essential to consider how poor shoulder mobility and stability can contribute to these issues. What Are Tennis and Golfer’s Elbow? Tennis Elbow Tennis elbow affects the outer part of the elbow, causing pain and tenderness on the outside. This condition typically arises from overuse of the forearm muscles, especially those responsible for wrist extension. Activities such as painting, or even prolonged computer use, or overstreching of extensor muscles can trigger this condition. Golfer’s Elbow Conversely, a golfer’s elbow affects the inner part of the elbow, leading to pain on the inside. This condition is commonly associated with activities that require gripping, flexing the wrist, or repetitive forearm movements, such as golfing, throwing, or lifting. In this presentation is the common flexor tendon that get’s irritated, and refer with pain. The Connection to Shoulder Mobility and Stability While tennis and golfer’s elbow are localized conditions, they often stem from dysfunctions higher up in the kinetic chain, particularly in the shoulder. Poor shoulder mobility and stability can lead to compensatory patterns that place undue stress on the forearm and elbow joints. Shoulder Mobility Limited shoulder mobility can restrict the natural range of motion for various activities. For instance, if your shoulders lack mobility, you may overcompensate with your forearm muscles during tasks that require reaching, lifting, or throwing. This overcompensation can lead to strain, resulting in conditions like tennis or golfer’s elbow. To maintain proper shoulder mobility, you want to ensure the use of the glenohumeral joint along your exercises and move it with specific drills, as this would stimulate the joint synovial fluid and maintain the joint lubricated. On the other hand, if the joint is hypermobile, we should look into how to stabilize it better. Shoulder Stability Shoulder stability is crucial for maintaining proper alignment during movement. Weakness in the shoulder stabilizers can cause the shoulder joint to become unstable, leading to altered movement patterns. When the shoulder isn’t stable, the body often compensates by engaging the forearm and elbow excessively, increasing the risk of injury. As mentioned in the paragraph above, this is what would occur when someone presents with a hypermobility body. In the hypermobility presentation, the ligaments are more lax and don’t hold back the joint movement as expected. Assessing and Addressing the Issue At Melbourne Massage and Treatment, we recommend a comprehensive approach to address tennis and golfer’s elbow effectively: Assessment of elbow epicondylitis Understanding the root cause of your pain is vital. During an initial consultation, we still mainly focused on your elbow presentation and addressed what movement reproduced the discomfort. But not only that. Throughout a tailored investigation, we will address what could be the root cause of the problem. This way, it would be easier to develop a tailored treatment plan. Treatment for elbow epicondylitis Massage Therapy: Targeted massage can alleviate tension in the forearm and improve blood flow, promoting healing. MDN: Myofascial Dry Needling plays a really effective role in tendinitis management. It focuses on targeting the underactive muscles, restoring the neural connection between the central nervous system and muscle, and desensitizing the painful area. Mobilisation: Mobilisation is an ideal technique to address mobility issue, and improve the range of motion of a joint. For epicondylitis presentations, the mobilisation could focus on wrist, elbow or shoulder. This would be based on the finding along the assessment. Strengthening Exercises: In the exercise program, we will initially focus on exercises that can desitentize the elbow area, such as isometric holds, and then move to eccentric and concentric exercises. In this second step, we would already focus on specific shoulder mobility or stability exercises, as needed. Education Understanding proper biomechanics can empower you to make lifestyle changes that prevent future injuries. Giovanni will guide you through exercises and techniques to maintain shoulder health and prevent elbow pain. Conclusion Tennis and golfer’s elbow can be debilitating, but addressing shoulder mobility and stability is key to recovery and prevention. At Melbourne Massage and Treatment in Fitzroy North, Giovanni is dedicated to helping you achieve optimal function and well-being. If you’re experiencing symptoms of tennis or golfer’s elbow, don’t hesitate to contact Giovanni or Book Now your 15-minute free phone consultation to learn more about a personalized assessment and treatment plan. Together, we can work towards getting you back to the activities you love, pain-free. FAQ Q: What are tennis elbow and golfer’s elbow? A: Lateral epicondylitis, affects the outer part of the elbow, causing pain due to overuse of the forearm muscles, particularly those responsible for wrist extension. Common activities that can trigger it include painting and prolonged computer use. Medial epicondylitis, impacts the inner part of the elbow, leading to pain often associated with gripping, flexing the wrist, or repetitive movements like golfing or throwing. Q: How are shoulder mobility and stability related to these conditions? A: Poor shoulder mobility can lead to overcompensation by the forearm muscles during activities requiring reaching, lifting, or throwing. Similarly, weak shoulder stabilizers can cause the shoulder joint to become unstable, forcing the forearm and elbow to work harder, which increases the risk of injury. Both factors contribute to the development of tennis and golfer’s elbow. Q: What are the signs of limited shoulder mobility? A: Signs include restricted movement during overhead activities, difficulty reaching behind your back, and discomfort during routine tasks that involve lifting or throwing. These limitations can lead to compensatory movements that stress the elbow. Q: How do you assess tennis or golfer’s elbow at Melbourne Massage and Treatment? A: We conduct a thorough assessment that focuses on your elbow presentation, identifying movements that reproduce discomfort. This investigation also explores potential underlying issues related to shoulder mobility and stability, helping us understand the root […]

Mar
Range of Motion is the movement of a joint within a 3-dimensional space. For each joint, we expect a minimum and a maximum degree of movement. When to use a range of motion evaluation. Before performing a Myotherapy, Remedial Massage, or a Thai massage session, we check for a Range of Motion, also know as ROM. Checking for ROM is to establish the functionality of the joint and the muscles that surround it. For example, when a client walks in complaining of cervical pain, the first thing we look in too after the postural assessment is the ROM. A postural assessment is an evaluation of the skeletal structure. After that, we ask the client to do specific movements with their head. Like, Rotation side to side, flexion, extension, and lateral flexion. Indeed, these are the basic range of motion for the cervical area. What can this range of motion tell us? Well, depending on the essential mobility of the person, we expect a minimum and maximum range. Let’s say that the client has average mobility; we expect the range of motion of their cervical to be: Flexion (able to flex the head forward and leave a gap of 3cm between the chin and the sternum) Extension, we look in too 70° of movement Lateral Rotation we look in too 80° of rotation (the chin is nearly in line with the shoulder) Lateral Flexion we look in too 45°. If this post talks to you, book your next massage session by clicking here. Is the range of motion the same for everyone? A person with a hypermobile joint range may have a 10° about less ROM than this. Indeed, a person that has a hypermobile joint range can reach 10° furthermore. That’s why every person needs his evaluation. Moving forward, if the range of motion is limited, it could be a muscle tightness or a joint mobilization issue. The best approach for improving joint mobilisation is the Myotherapy treatment or Thai Massage. Both techniques relieve muscle tension and improve muscle tone and joint mobility. The release of tension from the muscle would improve the ROM. On the other hand, when we ask a client to do a ROM, we don’t look only for the length of movement. Quality of movement. For the quality of movement, we refer to how smooth the movement is. Is the client trying to compensate for the cervical rotation by flexing the head? Is the client compensating for the flexion by shrugging the shoulder? Indeed, the movement of a joint is the key to understanding what muscle is responsible for the pain, discomfort or limited ROM. Once we individualise the key muscle/s, we can address the issue. Different types of ROM. In conclusion, the ROM can be active, passive and resisted. The client itself does active ROM. Passive are ROM done by the therapist with no assistance in controlling the movement by the client. Reisted is ROM active done by the client, with a resistance force applied by the therapist again the client’s movement. Each of this ROM can tell us something different about the joint. Active is about muscle lengthening. Passive is about joint mobility (ligament and tendon) Resisted is about the strength of the muscle. We can’t use the Resisted if Active or Passive reproduces pain. That would not be safe. Regarding the Resisted ROM, the resistance is applied in 3 different levels. When the pain gets reproduced, we stop the test. Occasionally, an orthopaedic test can be performed too. Orthopaedic tests are specific tests to evaluate in specific the muscle involved in the limited ROM.