If you’re searching for lymphatic therapy in Fitzroy North, it’s common to see terms like Manual Lymphatic Drainage (MLD) and Lymphatic Massage used interchangeably. As a clinical myotherapist with specialised training in lymphoedema management (MLD since Nov 2021; lymphoedema therapy since Oct 2024, trained with the Vodder Academy), I am here to clarify exactly what these treatments are and why one is clinically recommended over the other — especially for conditions like lymphoedema or post-surgical swelling. In fact, the importance of understanding the difference between MLD and Lymphatic Massage is vital when you want results that matter, and not just temporary relaxation. What Is Manual Lymphatic Drainage (Vodder Method)? Manual Lymphatic Drainage (MLD) is a specialised technique developed by Emil and Estrid Vodder in the early 20th century, and it is characterised by gentle, rhythmic hand movements to stimulate the lymphatic system. The reason behind the gentle and light movement is to ensure that during the treatment, we can stretch the skin and let it recoil naturally; therefore, we stimulate the lymphatic system at its full potential. Therefore, MLD is not a “massage” in the spa sense, it’s intentionally structured to follow physiological lymphatic pathways to support lymph flow. Key points about MLD: Trained practitioners follow evidence-based protocols. Movements are light, rhythmic, and intentional, not vigorous. The “Vodder method” is internationally recognised and taught with strict standards. It is often integrated into Complete Decongestive Therapy for lymphoedema. One recent article explains the theoretical physiology and clinical context of MLD in lymphoedema management. Manual lymphatic drainage: the evidence behind the efficacy (PubMed) What Is Lymphatic Massage? “Lymphatic Massage”, on the other hand, is more of a broad term used in wellness settings, like a SPA or massage parlour. The wordling is really similar to Manual Lymphatic Drainage, and is often followed by promises of “encourage fluid movement” or “before and after photos” but: Technique quality varies widely by practitioner. Some methods use deeper pressure and general strokes. It’s largely relaxation-focused, not always aligned with lymphatic anatomy. It isn’t generally part of evidence-based protocols for clinical conditions. In short, MLD is a clinically structured intervention; lymphatic massage is not. Indeed, who promotes Lymphatic massage as a service, often don’t know the pathway of the lymphatic system, and can’t tell you the difference between a Lymphoedema or a Lipoedema, and it may try to sell the fact that Lymphatic massage would detox your body (I will write a blog soon about this detox topic, as it is one of the biggest scam in the health and beauty industry). Side-by-Side: MLD vs Lymphatic Massage In the table below is a summary and a comparison between MLD and Lymphatic Massage features. Feature Manual Lymphatic Drainage (Vodder) MLD Lymphatic Massage Based on lymphatic anatomy ✔ ✖ Evidence-aligned technique ✔ ✖ Suitable for lymphoedema management ✔ ✖ Commonly used post-surgery ✔ ✖/varies Practised by trained therapists ✔ ✖ (wide variation) Relaxation / general wellness ✔ ✔ Clinical Evidence: What Research Shows About MLD and Lymphatic Massage As with any form of therapy, even in the case of MLD, the clinical research on MLD isn’t perfect, but the PubMed literature supports its role when used correctly within clinical programs. Lymphoedema Management A randomised controlled trial (RCT) reported that women with breast cancer–related lymphoedema experienced significant limb volume reduction and improved symptoms with MLD as part of therapy. A comprehensive systematic review found mixed outcomes but noted MLD’s accepted role in conservative lymphoedema treatment and generally positive effects on swelling and quality of life when integrated with other therapies. Inflammation & Post-Surgery Support MLD is also used, and clinical studies provide evidence in the setting of postoperative swelling and pain with orthopedic and cosmetic surgery. Indeed, post-surgery, the body responds with inflammation and swelling, which passes the acute phase, and the clearance of infections is better when moved to ensure the best recovery. Why MLD Is Clinically Preferred for Lymphoedema When lymphatic transport is impaired, as in lymphoedema or after surgery, the goal is not just temporary fluid “movement,” but supporting lymphatic drainage physiology. Here’s what clinical practice guidelines emphasise: Targeted Stimulation MLD uses gentle but precise hand movements that align with superficial lymphatic pathways and node groups. These are designed to: reduce interstitial fluid accumulation, activate lymphangiomotoricity, and facilitate fluid transport without trauma. This principle comes directly from the Vodder methodology as taught by the Vodder Academy. Part of a Larger Management Strategy Especially in lymphoedema, MLD is one component of a broader therapeutic approach that includes: ✔ compression therapy✔ movement and exercise✔ skin care and infection prevention This integrated strategy has been shown to improve outcomes more than any single therapy on its own. Post-Surgical Considerations As discussed in more depth in another blog, when heading for cosmetic and orthopaedic surgery, the recovery process is caractherised by an acute phase of swelling. That’s just teh body dping its thing. But, as we move away from the acute phase, it is essential to ensure that the oedema is reduced. That’s where MLD and compression therapy are essential. In fact, unlike a typical deep massage: MLD supports lymphatic flow without stressing fragile tissues. Studies show gentler lymphatic stimulation improves swelling and trismus after surgery. That’s why many rehabilitation specialists recommend structured MLD over general “lymphatic massage” in this context. So, What Should You Choose? As per everything, I reckon that your choice has to be aligned with your goal. Therefore: If you need clinical-grade lymphatic support for lymphoedema, post-surgical swelling, or ongoing fluid dysfunction, choose Manual Lymphatic Drainage (Vodder method) delivered by a trained clinician. If you want general relaxation and mild fluid support, a lymphatic massage in a wellness setting might feel nice — but it’s not a clinical substitute for MLD in these conditions. Conclusion From A Clinical Practitioner At Melbourne Massage and Treatment, Fitzroy North, I integrate MLD with evidence-based clinical reasoning, and not just as a “feel-good massage.” My approach is rooted in training with the Vodder Academy and ongoing lymphoedema therapy practice. If you’re concerned […]
Monthly Archives: February 2026

Blog
MLD vs Lymphatic Massage: A Clinician’s Guide to What Works and Why
If you’re searching for lymphatic therapy in Fitzroy North, it’s common to see terms like [...]
Continue readingFeb

Blog
Shoulder Pain Isn’t Just a Shoulder Problem
Shoulder pain is one of those presentations that can stop you from enjoying your day. [...]
Continue readingFeb

Blog
Glutes strengthening – Time To Exercises
Here in Fitzroy North, at my Myotherapy Clinic and 1:1 fitness class studio, I get [...]
Continue readingFeb
Blog
Calf Injury Melbourne – How Can Myotherapy Help With Rehab?
Calf injuries, such as a muscle tear, can be annoying to deal with because they [...]
Continue readingFeb
Blog
SWEP Program for Lymphoedema: What My Patients Need to Know
In Victoria, Lymphoedema patients are entitled to access the SWEP program (State Wide Equipment Program), [...]
Continue readingJan
Feb
Shoulder pain is one of those presentations that can stop you from enjoying your day. Rolling in bed becomes difficult; carrying shopping or even sitting there and doing nothing can be frustrating. At Melbourne Massage and Treatment, I got to see many clients who complained of shoulder pain for a variety of reasons. Although one thing that is common with those different types of pain is the imbalance in the mobility stability joint chain, especially in people who do physical labour, repetitive overhead work, or intense gym training. Therefore, while many people expect me to focus only on the sore spot in the shoulder, my myotherapy approach is always broader and more thorough. Yes, I treat the shoulder as the primary concern, but effective, long-term relief comes from understanding why your shoulder is overloaded in the first place. That means looking beyond the glenohumeral joint and assessing thoracic mobility, scapular control, and thoraco-scapular stability, which are key components that are often overlooked but critical for shoulder health and to help you fix the shoulder pain. Why Shoulder Pain Often Persists The Shoulder is a joint characterised by a great amount of mobility and not much stability, which puts it at high risk of injury and so pain. When your shoulder hurts, it’s rarely because the shoulder itself is “weak” or “damaged” in isolation. Indeed, to arrive to the pain response, either you had a severe trauma, like a fall on the shoulder or more commonly, the shoulder is compensating for: Poor thoracic spine mobility Weak or poorly coordinated scapular stabilisers Faulty movement patterns under load Repetitive strain from work or training And let’s be clear, we are all different, so two individuals who do the exact same job or sport may end up having different pain and presentation due to basic anatomical differences in the shoulder. That said, here are some common presentations that can lead to shoulder pain: If the thoracic spine doesn’t move well, the shoulder is forced to work harder. If the scapula doesn’t stabilise properly, the ac joint gets overloaded Genetically, the space between bonds (Humerus and Acromioclavicle joint) is narrower than the norm My Clinical Assessment Process For Shoulder Pain When you come to my Myotherapy Clinic in Fitzroy North for shoulder pain, I don’t just ask where it hurts, but I would assess: Thoracic spine mobility (especially rotation and extension) Cervical movement in active and passive motion Scapular positioning and control Shoulder range of motion under load Training or work-related movement demands Previous injuries or recurring pain patterns This is particularly important if you: Work in trades or manual labour Train heavily in the gym or sport Perform repetitive overhead movements Have had recurring or long-term shoulder pain A tailored assessment, such as the above one, allows me to not only pinpoint why the shoulder is in pain and what further investigation may be needed to confirm the findings but also address these factors, allowing us to understand the underlying drivers of your pain. The Role of Thoracic Mobility in Shoulder Pain The thoracic spine (mid-back) plays a massive role in how your shoulder functions. This is because the thoracic section of the spine is the mobile portion that anticipates the stable scapula-thoracic joint in the mobility, stability chain. Limited thoracic mobility can lead to: Reduced the overhead range Increased strain on the rotator cuff Poor scapular mechanics Neck and shoulder tension As part of the myotherapy treatment protocol for shoulder pain, I often combine manual therapy, joint mobilisation, and movement-based rehab to restore thoracic movement.When the thoracic spine moves better, the shoulder doesn’t have to overwork, pain reduces, and then we can increase the strength by increasing the load. A classic example of the thoracic shoulder relation is a cricket player. The thoracic rotation along the throwing action is essential to optimise the force imprinted during the throwing action. In fact, imagine the thrower in a cricket game, using only the shoulder, and not rotating that thoracic joint chain. The shoulder load would be excessive, and in a short time, it would cause overload injury and so shoulder pain. Scapular Stability: The Missing Link Your scapula (shoulder blade) is the foundation for shoulder movement. Indeed, the scapula-thoracic joint is the stable joint between the thoracic and the glenohumeral mobile joints. But not only that, indeed, the scapula is the origin point of the rotator cuff muscles, a group of muscles that control the positioning of your humeral head in the glenoid fossa. If it lacks stability or control: The shoulder joint becomes vulnerable Tendons are placed under excessive stress Pain persists despite “strengthening” exercises As a Clinical Myotherapist, I focus on improving thoraco-scapular stability, ensuring the shoulder blade moves smoothly and supports the arm during load, lifting, and rotation. This is especially crucial for people involved in: Weightlifting Cross-training Construction or trade work Sports requiring throwing or overhead movement To strengthen the stability of the scapula, we then have to work on the rhomboid muscles and the trapezius (upper, mid, and lower), but even the levator scapulae. So yes, it is not a quick fix to restore shoulder functionality and remove shoulder pain, but there is a step-by-step journey that can be taken, and it is your choice to start walking along this path. I am here only to help you understand what the right path is for your presentation and ensure we take the right route. Hypermobility and Shoulder Pain One often overlooked factor in shoulder pain is hypermobility. Hypermobility means your joints move more than the norms which isn’t always a bad thing, but it significantly increases injury risk when stability is lacking, particularly in the shoulder. For hypermobile individuals: Ligaments provide less passive support Muscles must work harder to stabilise joints Poor scapular stability leads to shoulder overload When hypermobility exists alongside poor thoraco-scapular stability, shoulder pain becomes far more likely. In these cases, treatment isn’t about increasing flexibility; instead would be the opposite: Improving neuromuscular control Enhancing scapular […]
Feb
Here in Fitzroy North, at my Myotherapy Clinic and 1:1 fitness class studio, I get to work with a wide range of clients, and what I notice is that there is a lack of knowledge and awareness on how to deliver a Glutes Strengthening. And why I believe that a squat is important is simply because squatting is an action that we do so often throughout the day that we all should be good at it, and it is the best functional movement that allows you to reinforce the full body structure. Therefore, when I come across those presentations, I ensure to educate my patients about the basic mechanics of a squat, including mobility, stability, and glutes strengthing. Are You Looking Into Glutes Strengthening? Let’s Check Your Joint Mobility and Stability First In order to deliver effective training for your glutes, including delivering an efficient squat, you will look at: Adequate ankle mobility A well-coordinated hip hinge Stability in fee tarsals and knee joints Those are regular things I would look at during a myotherapy treatment and 1:1 fitness class in Fitzroy North, to improve glute activation, movement efficiency, and injury resilience. Ankle Mobility Exercise to Improve Squat Depth and Lower Limb Mechanics As discussed in greater depth in the mobility and stability blog, before we start looking at strength and start working on functional movement, like the squat, we want to ensure that the mobile joints are mobile enough to deliver the right mechanics. In fact, limited ankle mobility often results in compensatory strategies such as: Excessive forward trunk lean during squats Early heel lift Increased stress on the knees or lumbar spine Clinical Importance of Ankle Mobility Adequate ankle dorsiflexion allows improved tibial progression during squatting movements, enabling more effective hip and glute loading. Exercise: Knee-to-Wall Ankle Dorsiflexion Drill Position the foot flat on the ground, facing a wall Aim for a 10 cm distance between the big toes and the wall Maintain heel contact with the floor Drive the knee forward toward the wall under control Perform slow, controlled repetitions Your aim is to teach the wall with the kneem, with a big toe-wall distance of min. 10 to 12 cm Clinical application:This exercise is commonly prescribed in myotherapy sessions to improve squat mechanics, reduce compensatory loading, and support long-term joint health. Hip Hinge Drill for Posterior Chain Activation and Spinal Control The hip hinge is a fundamental movement pattern required for safe and effective loading of the gluteal muscles, but not only that, indeed, poor hip hinge mechanics often present as excessive lumbar flexion or extension during deadlift-based movements. Why Hip Hinge Mechanics Matter Efficient hip hinging can help with: Increases glute and hamstring activation Reduces lumbar spine strain Improves RDL and deadlift performance Exercise: Wall-Assisted Hip Hinge Drill Stand approximately 20–30 cm from a wall Push the hips posteriorly to make contact with the wall Maintain a neutral spine and rib position Return to standing using glute contraction (squeeze those glutes) Clinical focus:This drill is a key component of both rehabilitation and performance-based programming at Melbourne Massage and Treatment. It is also a fundamental movement pattern taught in my glute-focused fitness classes, ensuring clients build strength safely and efficiently. Stability Starts From Your Feet Foot stability is a crucial part of delivering a good squat, especially during a low-bar squat, when feet are flat on the ground. Imagine your feet unable to give a stable direction to whatever is above, like the ankle, knee and hip. This would lead to knee shaking during squatting, and once the squat load increases, the risk of injury rises. So for foot stability, we look at: Even weight distribution of your load along the plantar of the feet, not only on your toes or on the heel. All toes, grabbing the floor, throughout the squat performance Lower-bar squat, feet flat on the floor (be barefoot or use gambaletto type of shoes) and feet wider than hip, stand in slight external rotation High-bar squat, feet open wide as hip stand (so a narrow stand) and heel well elevated. In both my clinical work and my strength-based fitness classes, foot stability is always assessed first. On the other hand, more about the high and low bar squat is available from this blog. Squats for Functional Glutes Strengthening In my glute-strengthening fitness class sessions, the squat is one of the primary movements we refine. Keep in mind that when we talk about squat for glut strength, we always refer to the lower-bar squat. Therefore, when performed with appropriate technique, this exercise is the most effective exercise for developing functional glutes strenghtening and improving lower-limb coordination. Below, you will find the most common Clinical Faults in Squatting Limited ankle mobility restricting depth Poor hip control resulting in lumbar compensation Reduced gluteus contribution due to motor control deficits So this is what you need to focus on to for a Optimal Glute Engagement while squatting: Maintain even foot pressure throughout the movement Maintain spinal alignment and controlled descent Drive upward through the heels and mid-foot Clinical note:Squat depth should be dictated by movement quality rather than arbitrary range targets. Romanian Deadlifts (RDLs) Another Glutes strengthening Exercise The Romanian deadlift, in comparison to the conventional deadlift, is a partial movement, where the load never touch the ground throughout the exercise (once it gets picked off the ground). This type of lift is ideal for exercising the posterior chain, particularly in the gluteal and hamstring musculature. Benefits of RDLs in Myotherapy and Strength Training Enhances glute and hamstring load tolerance Improves hip-dominant movement capacity Reduces injury risk through controlled eccentric loading RDL Execution Guidelines Maintain close bar or weight proximity to the body Initiate movement via hip hinge, not knee flexion Maintain spinal neutrality throughout the range Terminate the movement when pelvic control is lost Clinical relevance:RDLs are regularly integrated into rehabilitation and strength programs for clients with lower back pain or who are returning to lifting after injury. But are also ideal to build […]
Feb
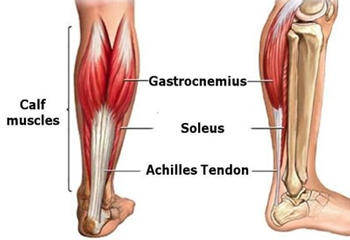
Calf injuries, such as a muscle tear, can be annoying to deal with because they can affect how we move and walk. This type of injury is common in runners, but can affect any person who may take part in a hit-class or go off for an occasional run, without proper athletic preparation. As a Myotherapist in Fitzroy North, my approach to calf injury rehab combines: Hands-on myotherapy Load management strategies Progressive exercise rehab Fitness-based rehabilitation classes What is a calf muscle tear? To start with, we need to understand which muscles make up the calf and which are most likely to tear. Calf muscles include: Gastrocnemius (medial head) Gastrocnemius (lateral head) Soleus Plantaris Tibialis posterior Flexor hallucis longus Flexor digitorum longus Fibularis (peroneus) longus Fibularis (peroneus) brevis Fibularis (peroneus) tertius The gastrocnemius (medial and lateral head) and soleus muscles are indeed the muscles that are most likely to tear, given the high load of work they do for ankle plantarflexion. These injuries commonly happen during: Sprinting or sudden acceleration Jumping or rapid change of direction Fatigue, poor load management, or inadequate warm-up Common symptoms include: Sudden sharp pain in the calf Tightness or cramping sensation Swelling or bruising Reduced push-off strength when walking or running When we look into the recovery approach, regardless of the injury severity, calf tears respond best to active rehabilitation rather than prolonged rest. How Myotherapy Can Help With Calf Muscle Tear? Myotherapy is a hands-on approach to musculoskeletal injury, and we not only look at massage as a form of treatment but also actively show you how to load your injured calf to rebuild the resiliency and strength needed to recover and prevent further injury. In summary, myotherapy can help by: Reducing excessive muscle tone via massage and or dry needling Improving circulation Supporting movement efficiency Addressing compensations in the ankle, knee, and hip Create a step-by-step exercise guide for your rehab protocol In fact, rehab isn’t just about pain relief; it’s about building capacity for better performance in everyday life. Calf Injury Rehab: A Step-by-Step Approach Calf injury, as mentioned earlier, is really common in active and not active patients, and therefore it is important to look at the clinical history of the patient, including the load those muscles go through in everyday life, the mechanism of injury, the mobility capacity and what the patient expects from the recovery process too. Indeed, at Melbourne Massage and treatment, I focus on: Individual assessment Pain-guided progression Gradual return to sport, work, or training If you’re searching for calf injury treatment in Melbourne, structured rehab with a myotherapist makes a real difference. Acute Calf Injury Management: PEACE & LOVE Acute or early-stage calf injury rehab follows the PEACE & LOVE framework rather than outdated RICE protocols. PEACE – First 1–3 Days After Injury Protect – Avoid excessive loading that may worsen the tear. Elevate – Elevation assists in swelling reduction. Avoid Anti-Inflammatories – Inflammation plays a key role in tissue healing. Compress – Light compression may help manage swelling. Educate – Understanding recovery timelines improves outcomes. LOVE – Subacute Phase and Beyond Load – Gradual loading improves tissue strength and tolerance. Optimism – Positive expectations support recovery. Vascularisation – Gentle pain-free movement improves circulation. Exercise – Progressive rehab restores function and confidence. In the acute phase, which lasts about 72 hours, we call it the inflammatory phase, and pain, redness, and swelling are expected Rest is recommended to let the body kick in its own healing capacity. Phase 1 Rehab: Isometric Calf Exercises As in most musculoskeletal injuries, once pain settles, even in the case of a calf injury, the first step to take in the rehab process is isometric exercises. Isometrics involve muscle contraction without repetitive movement, making them ideal for early healing. Benefits of isometric calf loading: Maintains strength Reduces pain Minimises stress on healing fibres Common examples: Standing calf press into the floor – works well for both the gastrocnemius and soleus muscles Seated calf holds – focus onthe soleus muscles Wall-supported calf contractions – if equilibrium is an issue Pain should remain low and settle quickly after exercise. A formula that I use with my patient is: pain post exercises = worst pain from injury / 2 So if your worst pain given by the calf injury was 8/10, post-isometric exercises, we are happy if you get a 4/10, but no more. And as long as it takes few minutes to 24 to settle, it’s fine. We will touch base on “why?” at the end of this blog. Phase 2 Rehab: Concentric and Eccentric Strengthening Week 1 to week 2 have passed since the injury, and it’s time to start loading the calf muscles with dynamic strengthening. The second phase is the longest one, and it may last somewhere between 4 and 5 weeks. Concentric loading The muscle shortens while producing force – Rising up during a calf raise Eccentric loading The muscle lengthens under load – Slow controlled lowering from a calf raise This phase restores: Calf strength Tendon resilience Capacity for walking, running, and work demands Isometric training allows the muscle fibres start the healing process, start closing the gap post calf tear, and therefore, now, with the strength training, we aim at improving the calf muscle function and injury resilience. This phase focuses as a priority on calf muscles, via calf raises, with a series of progressions: From double leg to single leg From feet flat on the ground to standing on a platform with a heel, with free fall From body weight only to increase the load From low reps to higher reps On top of those progressions for specific calf exercises, we will include other types of exercises, which focus on: Ankle mobility Quads and hamstring exercises to improve knee stability Glute exercises per equilibrium and power That said, at my Fitzroy North clinic, I ensure to pass on this information to my clients, teaching them the importance of tailored load, tempo, and volume to their […]