
Bone density is a key factor in bond fracture prevention. Bone is made of cells that die and regenerate. When this process is compromised, the risk of fracture arises. During the early stages of life, we can ensure that we intake and store calcium through food to build up our bones, but after a certain age (about 30), the body stops absorbing calcium, and the storage that we created is now our reserve for the rest of life. Cell Regeneration in Bone and Other Body’s Tissues The body’s cells, like muscle cells, skin cells, tendon cells, ligament cells and even bond cells, are in constant change via a process called cell regeneration. Old cells die off and they get replaced with new cells. In the case of bone, the cells that allow this process to happen are called osteoblasts. While we age, this process slows down, meaning that cells would still die, but they don’t get replaced. A typical example is a woman going through menopause. Estrogen, which is the hormone responsible for bond metabolism, allows the activity of osteoblasts. During menopause, indeed, women have a drop in Estrogen production, and osteoblasts are not as operative as they used to be. Strength Exercises and Cell Regeneration As this meta-analysis shows, strength exercises are a positive stress stimulus for the body and can help the osteoblast work harder and maintain bone cell regeneration. When the body perceives stress as physical resistance, it does its best to establish a reparation mechanism. So whenever we pick a weight against gravity, the body would implement a regeneration of the tissue that are used to complete this action. Who Is at Risk of Losing Bone Mass? There are several factors that can contribute to decreased bone mass: Age: Bone density typically peaks in early adulthood and declines with age. Gender: Women, especially postmenopausal, are at higher risk due to hormonal changes that accelerate bone loss. Family History: A family history of osteoporosis can increase risk. Body Size: Individuals with smaller body frames may have less bone mass to draw from as they age. Hormonal Levels: Thyroid imbalances and reduced sex hormones can lead to bone loss. Dietary Factors: Low calcium and vitamin D intake contribute to diminished bone density. Lifestyle Choices: A sedentary lifestyle, excessive alcohol consumption, and smoking are linked to weaker bones. I have included factors like dietary and hormonal levels in the above list. Bear in mind that taking supplements such as calcium and vitamin D (which helps retain calcium) could have severe contraindications. So, always talk to your doctor or specialist about the intake of supplements. How to determine Bone Density? To determine bone density, there is a diagnostic test called Dual-energy X-ray Absorptiometry (DEXA or DXA). This non-invasive procedure measures the mineral content in bones, usually in areas like the spine, hip, or wrist, to assess bone density and identify potential risks of osteoporosis or fractures. The results are given as a T-score, which compares your bone density to the average peak bone mass of a healthy young adult. A T-score of -1.0 or above is considered normal, while a score between -1.0 and -2.5 indicates low bone mass (osteopenia), and a score of -2.5 or lower suggests osteoporosis. Other methods, like ultrasound or quantitative computed tomography (QCT), can also assess bone density, but DEXA remains the gold standard for bone health evaluations. Mobility before strengthening So far, we have discussed how strength exercises are a good way to maintain bond density. Still, I would not recommend that anyone who is not into strength exercise and has bone density issues go and start lifting heavily. Why (?), you may ask. Well, before we start lifting heavy, we want to ensure that the body mechanics are optimal for it, so we better start looking into your mobility and then pass on to the strength part of things. Please be aware that mobility has nothing to do with elasticity or stretching. Those are different practices. How Can We Achieve Great Mobility For people who decide to take a journey to ensure an optimal level of mobility and then strengthen the body, the first step is to assess their joint mobility with active and passive range of motion. After that, we could use a combo of Myotherapy treatment and mobility exercises to ensure they can quickly pick up the best of their mobility capacity, given their subjective presentation. And here is a list of mobility exercises which we may look into at first: Hip Openers to improve range of motion in the pelvis and lower back. Ankle Drills to support proper weight distribution in weight-bearing exercises. Thoracic Spine Mobility Exercises to prevent excessive strain on the lower back. AC Joint External rotation to ensure we can build strong rotator cuff muscles, essential for shoulder health It Is Time To Strength. How Can We Do This? Once the minimum mobility is achieved, which may take 1 to 2 weeks of training, depending on each individual and their subjective history and effort, we can start looking into more strengthening exercises. So, here is a list of different exercises that can help with strengthening, written with the progressions to follow: Calf raises with double leg, single leg and weight Hamstring and Quads Curl that gets weight added as weeks go by Standing Adduction and Abduction at cable machine or with resistance bend Glut Muscles training at cable machine or with resistance bend Deadlift for back and posterior chain muscle strength Squat with weights and explosion variations Cuff rotator-specific strength is Ideal before stepping into more complex arm weight-lifting Cervical muscle strength to prevent cervical headache and sore neck All of those exercises, except the cervical one, can then be modified to achieve plyometric drills and combined movement. But this is a process that would take months, and there is no rush to get to it, as I want you to be safe throughout the entire journey. Integrating Exercise into Myotherapy Treatment At Melbourne Massage and Treatment, I incorporate […]
Tag Archives: massage technique

Blog
Chronic Venous Insufficiency and Swollen Legs: Compression Is The Way To Go
In Australia, Chronic Venous Insufficiency (CVI) affect more women than men, with a ratio of [...]
Continue readingMar

Blog
It Is Never Too Late To Join A 1:1 Fitness Class
At Melbourne Massage and Treatment in Fitzroy North, as a clinical Myotherapist, I am enthusiastic [...]
Continue readingMar

Blog
MLD vs Lymphatic Massage: A Clinician’s Guide to What Works and Why
If you’re searching for lymphatic therapy in Fitzroy North, it’s common to see terms like [...]
Continue readingFeb

Blog
Shoulder Pain Isn’t Just a Shoulder Problem
Shoulder pain is one of those presentations that can stop you from enjoying your day. [...]
Continue readingFeb

Blog
Glutes strengthening – Time To Exercises
Here in Fitzroy North, at my Myotherapy Clinic and 1:1 fitness class studio, I get [...]
Continue readingFeb

Oct
Mobility is the degree to which a joint can move before being restricted by surrounding tissues. Not all the joints taught are considered mobility joints. The Mobility and Motility Joints Theory Starting from the big toes joint and moving up the body to the upper cervical joints, we can count one by one a mobility joint alternating with a stability joint. So this would be like this: Big toes – M. Metatarsal – S Ankle -M Knee – S Hip – M Lumbar -S Toracic – M Lower Cervical – S Upper Cervical – M Shoulder – M Elbow – S Wrist – M Tarsal – S Fingers – M The major differences are: A Muscular structure surrounds mobility joints Stability joints are surrounded by ligaments and tendons Mobility joints move in more planes than stable ones. The stability joints, indeed are essential to the body mechanics to ensure that gravity and force applied to the body by its own weight are well distributed. First thing first. Now, if we plan to strengthen our body, like by going to the gym, running or doing any sports activity, ideally we would like to ensure that the mobile joints can deliver the minimum required of ROM. Why? Well, if the mobility joints are stiff or not mobile enough, the priority of moving would not diminish and the stability joints, are going to do their best to compensate. But let’s see this with an example. Mark (name of fantasy) who is an office worker, spends about 40 hours a week at his desk, and to reduce the work and life stress decided to start a routine run 3 to 4 times a week for 1 hour per time. Mark thinks that to go for a run, you don’t need training and has no clue about the mobility, stability and strengthening chain. After a few weeks that is enjoying his new routine, Mark start experiencing knee pain. Mark also didn’t realise that due to the long hours of sitting at the office, his hips joint are tight, and his external rotators, such as the gluteus max and piriformis, are tight. As per consequence, when Mark stands up, the angle of the gate (AOG), which refers to the rotation of the foot in a standing position, is up to 4 toes per side. (3 toes is the max AOG we expect in the foot). Now, what happens next is that when Mark goes running, his ankle mobility and hip mobility are visibly restricted. So, he will lean forward with the upper body, by having tight hips, and strike the floor with the feet externally rotated, so all the body weight will be loaded in the middle of the foot. As a result, the Stability Joint that sits between the ankle and hip, so the knee, will compensate for the other two joint dysfunctions. In this case, the knees would take extra pressure medially and stretch out laterally. So, what should Mark do?! Well, initially, to stop the pain from happening, stopping running would be a good idea. Said so, that would not fix the problem. What Mark should do, is: Massage to boost the change within the tight joints and reduce the knee pain Start a mobility program to improve the Hip and Ankle functionality Exercises that aim to reduce tension in the external rotator reinforce the internal rotator (Gluteus Med and Min) Train on how to run These are the basic steps to implement a model of Mobility, Stability, and Strengthening. Does this model apply to other sports activities? Of course, it does. Visualise your body as a giant mechanical machine made of rope and hinges. The mechanical result will not be ideal if the hinges are stiff and the ropes are tight. To improve the result, each component needs to be looked after. So what message would be the most recommended? Along with Melbourne Massage and Treatment services, Thai Massage, Remedial Massage, and Myotherapy are soon the most recommended services Giovanni offers to improve the body’s mobility. Regarding mobility training, Thai Yoga is also an effective way to improve joint mobility, as these exercises focus primarily on improving joint mobility. What there is to consider is the patient’s presentation, medical history and pre-existent injuries. If there are no significant concerns, I suggest Thai Massage as the best approach. For people who have presentations such as Diabetes n1 or hypertension, Myotherapy treatment or Remedial Massage is mainly recommended.

Oct
Joint mobilisations are manual therapy techniques that improve joint mobility and flexibility and reduce joint pain. Joint mobilisation can be applied to many body joints. Some contraindications have to be taken into consideration for mobilisation: Joint swelling Osteo Arthritis Bone Fracture Bulge disk (if the mobs are intended on a vertebra) Mobilisation VS Adjustment. Mobilisations are different from Chiropractic adjustment. The difference is that Chiropractic adjustments are fast movements applied with more significant pressure. Mobilisations are constant slow, repetitive movements applied to the joint. Along with a Myotherapy treatment, Giovanni would evaluate if mobilisation is the proper treatment for your condition. For example, mobilisation along the spine is recommended when someone presents with a stiff back in the sacrum, lumbar, thoracic or lower cervical area. Giovanni would always double-check with you about what the mobs felt like. Types of Mobilisation. As we already know, the body is made of different types of joints. Given the different types of joints, like socket joints, plane joints and more, others are the type of mobilisation. For example: For a joint like the hip, we can apply mobility like a distraction, anterior-to-posterior pressure or posterior-to-anterior pull, internal rotation or superior-to-inferior pull. Some of these techniques can be applied to other joints, and each way of using a mobilisation aims to improve a specific range of motion. So, all up, the type of mobilisation that we have are: Superior to Inferior; Inferior to superior; Distraction; Posterior to Anterior; Anterior to Posterior; Posterior glide; Anterior glide; Lateral glide; Medial glide. Mobilisation Belt. A mobilisation belt can be used to deliver the mobilisation based on the joint we aim to work on. A belt is a tool wrapped around the designated joint we want to work on and is used to apply stretches that would not be as easy to achieve by hand. An example is a hip distraction. For distraction, we refer to it as a force that pulls a joint apart. In the case of a hip, the head of the femur is pulled away from the hip’s socket from the medial to the lateral direction. As you would imagine, using bare hands for applying this technique not only could result in an uncomfortable approach to the intimacy of the patient, but it would requireFr too much effort for the therapist, resulting in poor mobilisation delivery and risk of injury. Therefore, the best tool is a belt wrapped around the patient’s hip and the therapist’s waist. Why use the mobilisation technique? The mobilisation technique aims not to reproduce pain, cracking sound, or sharp sensation. Indeed, the aim is to reproduce a firm pressure/pull on the joint area. Regarding the thoracic area, if any of those vertebrae reproduce pain or sharp sensation, applying the mobs along the vertebrae/ribs joint would be better. Doing so would still possible to affect spine mobility indirectly. Giovanni’s training for this type of modality started during the Advance Diploma in Myotherapy at RMIT and continued at the Bachelor of Health Science at Torrens University. Mobilisations technique can be applied to Big Toe, Ankle, Shoulder, Feet, Hip, Wrist, Elbow, Vertebrae, SIJ joint, Facet Joint, Clavicle and other body areas. An example of joint mobilisation for the feet. Mobilisations at the ankle area are used for improving ankle mobility. Indeed, improving ankle mobility is to better support during the walk, standing and or running. Always talking about the feet area, the mobilisation applied to the Big Toes is used along the Metatasolphalangeal Joint. Do you feel your joints stiff? Your booking for a Myotherapy treatment with Giovanni is just a click away. This mobilisation is applied by creating a distraction movement within the joint, pulling the toes away and then using it for passive flexion and extension. As mentioned in another blog post about wearing bear foot shoes, the Big toes are meant to extend from 65° to 70°. Conclusion The Big Toes are the feet joint that should push the most in the feet strike as we walk. In conclusion, mobilisations are a great way to increase mobility within a joint allowing better movement and improving the range of motion.

Sep
Myotherapy is a massage technique to treat or prevent soft tissue pain and restricted joint movement. “Myotherapy” stands for “Myo” Muscle “Therapy” therapy. In Australia, and specifically in Melbourne, it is a practice that took over the massage market in the last few decades and is not becoming more and more popular. There is Dry Needling and Joint Mobilization along the different techniques used in a Myotherapy treatment. Is Myotherapy Safe? Yes, Myotherapy is a safe treatment. Said so, you want to ensure that the therapist treating you has their qualification up to date. Here is a link to my qualification. What about Dry Needling in a Myotherapy Treatment? Dry needling is one of the many ways a Myotherapist can treat a client, but it is unnecessary. Before using needles, the therapist always has to double-check with the clients the following: No metal allergy No bleeding disorders No needle fear or phobia The client feels comfortable with such treatment The therapist does explain how dry needling works Is Myotherapy available at Melbourne Massage and Treatment? Yes, it is. I am a fully qualified Myotherapist who completed an Advance Diploma in Myotherapy at RMIT University. On top of all, I am now enrolled in the last year of my Bachelor’s Degree in the Myotherapy Clinic at Torrens University. What’s the difference between Myotherapy Treatment and Remedial Massage? Myotherapy is similar to a Remedial Massage session. The difference is that a Myotherapist has more knowledge about the human anatomy, joints, and functionality. So before the session, the therapist would guide the patient through a specific range of motion to evaluate the body’s presentation. Done so, the therapist has an idea of what can be done to improve the body’s presentation. Furthermore, a Myotherapist is trained to use mobilization, which is a repetitive joint movement to improve the joint’s range of motion. My favourite “mobs” are along the spine. They consist of a gentle push over the transverse process of the spine. Applying this constant firm push, the transverse process gain mobility, allowing all the muscle inserts originating from that joint to be more mobile. Is a mobilization the same as what a chiro does? No is not. The Chiro makes an adjustment, which is a fast joint pull or push, to adjust its position or functionality. Along with an adjustment, the patient has no control over the fast movement. Indeed, during mobilisation, the patient can take control of the push and stop the treatment if he/she does feel uncomfortable. Book Now your Myotherapy treatment with Giovanni. Giovanni is available in Fitzroy North at 175 Holden St Monday to Saturday 9 am to 7pm.
Muscle and Tendon are two types of fibres that connect bonds, allowing the joint to be moved by contracting or extending. Muscles and Tendons characteristics. A muscle consists of fibres of muscle cells covered by fascia, bundled with many more fibres, surrounded by thick protective tissue. So each muscle fibre is covered in the fascia, then wrapped as a whole muscle in more fascia. A tendon is a high-tensile-strength band of dense fibery connective tissue. Indeed tendons can transmit the mechanical forces of muscle to the skeletal system. Tendons, as per ligaments, are made of collagen fibres. Compared to a tendon, a muscle is elastic and sits in between 2 tendons parts which keep the muscle itself connected to bonds. So yes, muscles are not directly connected to bond themself. Luckily, there is to say, because if this was the case, it would be really easy to suffer from injuries like a muscle tear. Said so, it is now easy to understand that tendons are capable of holding more force. Injury type Due to the consistency of the tendon and its functionality, we can now understand why a tendon tear or rupture is a severe injury that requires surgical intervention and months of rehabilitation. On the other hand, often, after months of rehabilitation, still, the tendon would not go back to its original state. A common tendon rupture is Achille’s tendon. Achille’s tendon connects the lower part of the Gastrocnemius and Soleus to the foothill. Repetitive movement and repetitive partial load on this tendon are the leading cause of injury. Healthy muscle and tendon Simple and gentle exercises are a good way to keep your muscle and tendon out of trouble. The key points of these types of exercises are: Consistency Resisted load (by using rubber bands) Starting with light weight to then building up with time heavier load Good posture doing the exercises Have a day of rest from exercises once a week Avoid exercises that aggravate your pain. Said so, other critical points for muscle and tendons good health seating into: Having a good night’s rest Eating more fresh food than overprocessed food Regarding recovery from an injury, as previously mentioned in the ice pack and/or heat pack posts, the usage of temperature is recommended based on the stage of the injury and the pain experienced with it. Even though on an inflamed tendon, never apply a heat pack. Are you in need of treatment? Don’t look any further, and book your initial consultation by clicking here.

Jul
In a previous blog, we did talk about heat packs, now it is time to talk about the Ice Pack. Ice pack application, in the last few years, is a practice that got reviewed. What Ice Pack is about? An Ice pack, as the name says, is a cold (icy) bag. As better explained in this study an ice pack is something that can be applied to an acute injury, to prevent swelling and reduce pain, but it can’t be used for too long. As per the heat pack, an Ice Pack burn the skin, and that’s one reason why its usage has to be short (10 to 15mins at a time). In addition, extended exposure to icy temperatures, would reduce the blood flow around the injured tissue and can also damage nerves. Ice Pack usage recommendation: You have a new injury or aggravation of an existing condition, and the pain is above 7 out of 10. Where you want to minimize swelling to keep you mobile later. There are different types of Ice packs: Home-made one, ice from the freezer wrapped in a towel. Gel pack Ice Bag (as per the photo) Instant one – most of the time found in the first aid kit. Snap it and a chemical reaction would occur in the bag and freeze the bag. Those last ones are efficient as you can store them anywhere safely and use them as you need them. The cold lasts for about 20 minutes. Not to be used if they are broken. On the other hand, if you running out of ideas of what to use as a Cold pack, you can even use a bag of frozen food. Still would do the work. We have the ice bath and the cold show related to this topic. I did experience cold showers myself, most of the time not of my choice, but because of a limited supply of hot water, and I have to say that even on this topic, there are a series of debates on how that works and if it’s beneficial. So far, a cold shower, compared to a hot shower, is better for dry skin. This is because the heat of the water combined with soap can wash away the good oils of the skin. Then the benefit of an Ice bath can be more of a placebo effect. But again, I haven’t done much digging about myself, so I would stay out of any comment regarding it. Ice pack after a Massage? Well, as mentioned above, the usage of Ice Pack is suggested after an acute injury. So, either after a Remedial Massage or a Thai Massage, firstly there should be no acute injury, secondly, you want the blood flow along the worked area to stay active and not restricted. That’s why a heat pack would be more recommended. If you find this helpful information and need a massage, book your next session here.

Apr
A Scap-Off Load is a special test or functional test that we use to evaluate the implication of Lev Scapular and Up. Trap in Cercival Rotation. As previously mentioned, in cervical rotation, we got a fair bit of muscle working towards this action. As many clients come in with cervical pain, it’s time to explain in more detail what’s going on there. Cervical Rotation. How does it happen? So, when we rotate our head, either right or left, the muscle on the same side of the rotation movement is contracting. If a muscle along those is weak, we may reproduce pain in rotation along the same side. To thin down which muscle is responsible for the limited ROM, we have to safely deactivate some of them to see if the left behind one can deliver the expected movement. Here is an example of how scap offload works. If a client comes in with 30° Cervical rotation on the R and pain on top of the scapula, that could be an indication that its levator scapulae is the muscle to target. To confirm this hypothesis, I would ask the client to shrug their shoulders and flex their elbow (the client is sitting on a stool). After that, I will make my way behind the client, and I will support their shoulder weight with my forearm and hands. As the client relieves the shoulder tension, that lev scapulae and up. Traps. are now deactivated. The next thing would be to ask the client to perform the cervical rotation. Ideally, I would like to see the client have a full range of motion (80° to 90°). If this post talks to you, book your next massage session by clicking here. That would tell me that the only muscles that are limiting the cervical rotation are the lev scap. and up trap. On the other hand, what could happen, is that the cervical rotation is, yes improved, but still limited, compared to the ROM expected. In this case, the muscles involved in the stiff range of motions are not only lev scap. and or upper trap. In fact, what is causing the limitation is the cervical occipital muscles. And yes, spending long hours at the computer or looking at the phone doesn’t help. After this test, to narrow down even more which other muscles are involved in the stiffness of the cervical area, I do run another series of tests. Those tests would look into joint areas like C0-C1, which would refer to Obliquus Capitis Superior muscle, and the C1-C2 test, which would look at tension for Obliquus Capitis Inferior. Furthermore, for the other facet joints that make up the lower cervical region (C3 to C8), I would analyze each facet joint individually. These series of tests are indeed part of my Myotherapy training. Last would be then the usage of the joint mobilisation technique. In this case, we would look into what joint has lost mobility or which one has an excess of it. Strengthening the cervical. In order to improve the presentation, massage on its own is not enough. As per any condition so far, the strengthening of the muscle, in this case, the cervical and upper thoracic one, would allow to prevent further pain and discomfort. The work that the cervical muscle has to do daily is considerably high, giving the natural weight of the skull. So exercising a chin tag in a supine position can help. Ideally, we would do these exercises in the supine position (lying down face up) so that we have gravity to fight back as we train our deep flexors. To further improve the strengthening, once the chin tag is not enough, we can start using a soft rubber band to create resistance. Said so, be mindful that the cervical area is a delicate area to work on too, and those exercises are best practice under the supervision of an expert trainer or massage therapist.

Mar
As already mentioned earlier MLD is a fantastic manual technique that can be used to improve the healing of many conditions. Along with the conditions that MLD is useful for there is bone fracture. Said so, in order to understand how MLD can help to speed up the recovery from a bone fracture we have to analyse what’s happening within the body when such trauma happens. A bone fracture is an injury that can happen at any age, due to an accident or trauma. The main type of bone fractures are: Displaced Angulated Shortened Rotate Symptoms of bone fracture Pain Swelling Bruising Deformity Inability to use the limb. The fracture so can be a crack side to side or in the middle of the bone. Eventually, the bone can crumble too, or break in multiple areas. At the worst, the bone can also cut the skin, and come out of the body. If this post is talking to you, book your next massage session by clicking here. Depending on where the fracture is, and what type of fracture it is, surgery could be required. Independently if surgery is required or not, still MLD can help to boost the recovery. Indeed, when a fracture happens the body recognises a trauma to its system. As long as the body won’t know exactly what the trauma is, and if the trauma does involve a skin crack or not, to prevent infections and external bacteria or pathogens to enter the body, the vein, capillaries and the lymphatic system around the trauma area get restricted. As per result, the body does swell. In fact, this explains why, when oedema happens the body does swell. It is an automatic body response to prevent further damage to happen. As the body then, realise what the issue is, slowly does reactivate the lymphatic system, and does fully reopen veins and capillaries, so that the blood can start circulating again freely. But the time that the body can reduce the swelling by itself, with a lymphatic system that works at regular speed (about 7 to 8 bits per minute) it would take a while to reduce the swelling. Furthermore, when I bone is broken that body part would have to stay still for a while, weeks or months. As per result, the blood and lymph flow would be slower than usual. And here is where MLD comes to be useful. If by reading this post, you feel like MLD is what you need now to recover from your injuries, click here to book now your next session. As MLD therapists indeed, we would check that there is no acute infection in the area where we want to apply MLD. If that’s the case, then, we can start our work. By boosting the lymphatic system, up to 3 to 4 times its normal ratio, we can quickly reduce the swelling. And what about if the area affected is covered with a plaster cast? Well, let’s not forget that the lymphatic system works as a vacuum and the area of loads is below the clavicle. So, stimulating the Lymphatic system at the top can actually already improve its suction ability till down the feet. For example, if the fracture is at the foot, initially MLD can be applied at the neck, to open the Lymphatic System duct that reverses in the veins, and secondly can be applied to the abdominal level and down the legs, just before the foot. Now, that swelling reduction, come’s with many benefits. For example, in the area treated, there is a transaction of extra oxygen, protein, vitamins, blood and other essential elements useful for the bone to heal. And occasionally, depending on the type of fracture is not only the bone the one that has to heal. In fact, along with a bone fracture, the body part fractured stays steel for weeks and months. That would create a weakness in the muscle that would then require rehabilitation. As a Remedial Massage therapist, I would have to refer the client to a Physiotherapist for rehabilitation. Even so, as a Remedial Massage therapist, I can still deliver massage services that can help in restoring muscle functionality. In conclusion, MLD can help with: reducing the swelling along a bone fracture; help in speeding up the recovery of the skin damaged by the fracture and or by the operation; Speeding up the healing of muscles and soft tissue around the fracture; Ultimately, by increasing relaxation, MLD is also useful to keep the humour of the person at ease, as often happens that after a trauma such as a bone fracture, the person can feel anxious and demoralised due to poor mobility and difficulties in moving.
Mar
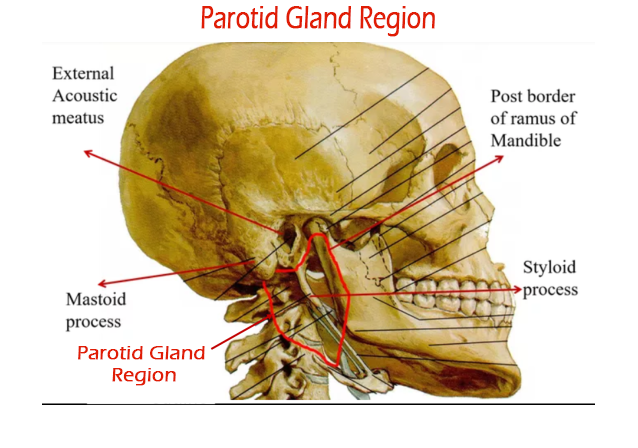
TMJ or Temporomandibular joint is bilaterally located on the side of the human head. TMJ and Movement Upper Compartment Protrusion Retrusion Lower Compartment Lower the Jaw Raise the Jaw Lateral Deviation Said so: the opening is the combination of Protrusion plus Lowering the Jaw closing the mouth is Retrusion plus Raising the Jaw. TMJ and Pain When TMJ is in pain, we can find it hard to talk, eat and sometimes even rest, as the pain can be pretty strong. Moving forward, not everyone knows that deep under TMJ we have what we call Parotid Gland. The Parotid Gland is a salivary gland, and if gets infected, it can swallow up and be quite painful. What can happen at the Parotid Gland is an accumulation of calcium in its duct, and saliva can’t be expelled. Even though viruses or bacteria can also be responsible for TMJ infection. What also most people are not aware of is that in the Parotid Gland, there are lymph nodes. TMJ and MLD. The fact that the gland can be swollen is an indication that fluid is stuck in it. MLD, thanks to the boosting of the lymphatic system, which is responsible for reducing swelling in the body, can be the perfect technique to reduce the swelling and so restore the functionality of TMJ. If this post talks to you, book your next massage session by clicking here. The Parotid Gland lymph nodes unload their Lymph Obligatory Load into the cervical nodes. So as per usual, at the start of the MLD treatment, we will work along the upper neck, medial neck and then the terminal (just between the clavicle and the upper trap). In addition, what makes a difference with MLD is that is a pain-free technique. That would allow the client suffering from TMJ pain to receive a treatment that would not aggravate the pain feeling and would end up giving a deep relaxation too. Other work techniques can be used, such as Myotherapy and Remedial Massage trigger point, or dry needling for Myotherapy treatment. The Remedial Massage TMJ treatment is a valuable technique but would not resolve the problem at the root cause. In conclusion, MLD is probably the best manual, not invasive treatment that can be done for TMJ. Talk to your dentist about this option, and if they are not aware of what MLD is, don’t be surprised, it is, yes an excellent technique, but it is still not well known by many practitioners, dentist included.

Mar
Range of Motion is the movement of a joint within a 3-dimensional space. For each joint, we expect a minimum and a maximum degree of movement. When to use a range of motion evaluation. Before performing a Myotherapy, Remedial Massage, or a Thai massage session, we check for a Range of Motion, also know as ROM. Checking for ROM is to establish the functionality of the joint and the muscles that surround it. For example, when a client walks in complaining of cervical pain, the first thing we look in too after the postural assessment is the ROM. A postural assessment is an evaluation of the skeletal structure. After that, we ask the client to do specific movements with their head. Like, Rotation side to side, flexion, extension, and lateral flexion. Indeed, these are the basic range of motion for the cervical area. What can this range of motion tell us? Well, depending on the essential mobility of the person, we expect a minimum and maximum range. Let’s say that the client has average mobility; we expect the range of motion of their cervical to be: Flexion (able to flex the head forward and leave a gap of 3cm between the chin and the sternum) Extension, we look in too 70° of movement Lateral Rotation we look in too 80° of rotation (the chin is nearly in line with the shoulder) Lateral Flexion we look in too 45°. If this post talks to you, book your next massage session by clicking here. Is the range of motion the same for everyone? A person with a hypermobile joint range may have a 10° about less ROM than this. Indeed, a person that has a hypermobile joint range can reach 10° furthermore. That’s why every person needs his evaluation. Moving forward, if the range of motion is limited, it could be a muscle tightness or a joint mobilization issue. The best approach for improving joint mobilisation is the Myotherapy treatment or Thai Massage. Both techniques relieve muscle tension and improve muscle tone and joint mobility. The release of tension from the muscle would improve the ROM. On the other hand, when we ask a client to do a ROM, we don’t look only for the length of movement. Quality of movement. For the quality of movement, we refer to how smooth the movement is. Is the client trying to compensate for the cervical rotation by flexing the head? Is the client compensating for the flexion by shrugging the shoulder? Indeed, the movement of a joint is the key to understanding what muscle is responsible for the pain, discomfort or limited ROM. Once we individualise the key muscle/s, we can address the issue. Different types of ROM. In conclusion, the ROM can be active, passive and resisted. The client itself does active ROM. Passive are ROM done by the therapist with no assistance in controlling the movement by the client. Reisted is ROM active done by the client, with a resistance force applied by the therapist again the client’s movement. Each of this ROM can tell us something different about the joint. Active is about muscle lengthening. Passive is about joint mobility (ligament and tendon) Resisted is about the strength of the muscle. We can’t use the Resisted if Active or Passive reproduces pain. That would not be safe. Regarding the Resisted ROM, the resistance is applied in 3 different levels. When the pain gets reproduced, we stop the test. Occasionally, an orthopaedic test can be performed too. Orthopaedic tests are specific tests to evaluate in specific the muscle involved in the limited ROM.
- 1
- 2