Shoulder pain is one of those presentations that can stop you from enjoying your day. Rolling in bed becomes difficult; carrying shopping or even sitting there and doing nothing can be frustrating. At Melbourne Massage and Treatment, I got to see many clients who complained of shoulder pain for a variety of reasons. Although one thing that is common with those different types of pain is the imbalance in the mobility stability joint chain, especially in people who do physical labour, repetitive overhead work, or intense gym training. Therefore, while many people expect me to focus only on the sore spot in the shoulder, my myotherapy approach is always broader and more thorough. Yes, I treat the shoulder as the primary concern, but effective, long-term relief comes from understanding why your shoulder is overloaded in the first place. That means looking beyond the glenohumeral joint and assessing thoracic mobility, scapular control, and thoraco-scapular stability, which are key components that are often overlooked but critical for shoulder health and to help you fix the shoulder pain. Why Shoulder Pain Often Persists The Shoulder is a joint characterised by a great amount of mobility and not much stability, which puts it at high risk of injury and so pain. When your shoulder hurts, it’s rarely because the shoulder itself is “weak” or “damaged” in isolation. Indeed, to arrive to the pain response, either you had a severe trauma, like a fall on the shoulder or more commonly, the shoulder is compensating for: Poor thoracic spine mobility Weak or poorly coordinated scapular stabilisers Faulty movement patterns under load Repetitive strain from work or training And let’s be clear, we are all different, so two individuals who do the exact same job or sport may end up having different pain and presentation due to basic anatomical differences in the shoulder. That said, here are some common presentations that can lead to shoulder pain: If the thoracic spine doesn’t move well, the shoulder is forced to work harder. If the scapula doesn’t stabilise properly, the ac joint gets overloaded Genetically, the space between bonds (Humerus and Acromioclavicle joint) is narrower than the norm My Clinical Assessment Process For Shoulder Pain When you come to my Myotherapy Clinic in Fitzroy North for shoulder pain, I don’t just ask where it hurts, but I would assess: Thoracic spine mobility (especially rotation and extension) Cervical movement in active and passive motion Scapular positioning and control Shoulder range of motion under load Training or work-related movement demands Previous injuries or recurring pain patterns This is particularly important if you: Work in trades or manual labour Train heavily in the gym or sport Perform repetitive overhead movements Have had recurring or long-term shoulder pain A tailored assessment, such as the above one, allows me to not only pinpoint why the shoulder is in pain and what further investigation may be needed to confirm the findings but also address these factors, allowing us to understand the underlying drivers of your pain. The Role of Thoracic Mobility in Shoulder Pain The thoracic spine (mid-back) plays a massive role in how your shoulder functions. This is because the thoracic section of the spine is the mobile portion that anticipates the stable scapula-thoracic joint in the mobility, stability chain. Limited thoracic mobility can lead to: Reduced the overhead range Increased strain on the rotator cuff Poor scapular mechanics Neck and shoulder tension As part of the myotherapy treatment protocol for shoulder pain, I often combine manual therapy, joint mobilisation, and movement-based rehab to restore thoracic movement.When the thoracic spine moves better, the shoulder doesn’t have to overwork, pain reduces, and then we can increase the strength by increasing the load. A classic example of the thoracic shoulder relation is a cricket player. The thoracic rotation along the throwing action is essential to optimise the force imprinted during the throwing action. In fact, imagine the thrower in a cricket game, using only the shoulder, and not rotating that thoracic joint chain. The shoulder load would be excessive, and in a short time, it would cause overload injury and so shoulder pain. Scapular Stability: The Missing Link Your scapula (shoulder blade) is the foundation for shoulder movement. Indeed, the scapula-thoracic joint is the stable joint between the thoracic and the glenohumeral mobile joints. But not only that, indeed, the scapula is the origin point of the rotator cuff muscles, a group of muscles that control the positioning of your humeral head in the glenoid fossa. If it lacks stability or control: The shoulder joint becomes vulnerable Tendons are placed under excessive stress Pain persists despite “strengthening” exercises As a Clinical Myotherapist, I focus on improving thoraco-scapular stability, ensuring the shoulder blade moves smoothly and supports the arm during load, lifting, and rotation. This is especially crucial for people involved in: Weightlifting Cross-training Construction or trade work Sports requiring throwing or overhead movement To strengthen the stability of the scapula, we then have to work on the rhomboid muscles and the trapezius (upper, mid, and lower), but even the levator scapulae. So yes, it is not a quick fix to restore shoulder functionality and remove shoulder pain, but there is a step-by-step journey that can be taken, and it is your choice to start walking along this path. I am here only to help you understand what the right path is for your presentation and ensure we take the right route. Hypermobility and Shoulder Pain One often overlooked factor in shoulder pain is hypermobility. Hypermobility means your joints move more than the norms which isn’t always a bad thing, but it significantly increases injury risk when stability is lacking, particularly in the shoulder. For hypermobile individuals: Ligaments provide less passive support Muscles must work harder to stabilise joints Poor scapular stability leads to shoulder overload When hypermobility exists alongside poor thoraco-scapular stability, shoulder pain becomes far more likely. In these cases, treatment isn’t about increasing flexibility; instead would be the opposite: Improving neuromuscular control Enhancing scapular […]
Tag Archives: myotehrapy

Blog
MLD vs Lymphatic Massage: A Clinician’s Guide to What Works and Why
If you’re searching for lymphatic therapy in Fitzroy North, it’s common to see terms like [...]
Continue readingFeb

Blog
Shoulder Pain Isn’t Just a Shoulder Problem
Shoulder pain is one of those presentations that can stop you from enjoying your day. [...]
Continue readingFeb

Blog
Glutes strengthening – Time To Exercises
Here in Fitzroy North, at my Myotherapy Clinic and 1:1 fitness class studio, I get [...]
Continue readingFeb
Blog
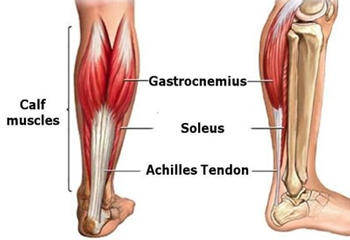
Calf Injury Melbourne – How Can Myotherapy Help With Rehab?
Calf injuries, such as a muscle tear, can be annoying to deal with because they [...]
Continue readingFeb
Blog
SWEP Program for Lymphoedema: What My Patients Need to Know
In Victoria, Lymphoedema patients are entitled to access the SWEP program (State Wide Equipment Program), [...]
Continue readingJan

Dec
Elbow tendinopathy, whether it presents as tennis elbow (lateral elbow pain) or golfer’s elbow (medial elbow pain), is one of the most common overuse injuries in active people, desk workers, and manual labourers. At Melbourne Massage and Treatment in Fitzroy North, I frequently help patients recover from both forms of elbow tendinopathy. Elbow Tendinopathy: How Does It Manifest? “Tendinopathy” refers to irritation and degeneration within a tendon due to repeated overload. Elbow Tendinopathy, in both of its forms, tennis or golfer’s elbow, can sound like a sport-related injury, but it has little to do with the sports world. The reason why those presentations carry their name is due to the sport action, which requires that specific muscle group to work to deliver the golfer strike (medial) or tennis strike (lateral). So what can actually cause an elbow tendinopathy are: Sudden increase of tendon load – lifting heavier than usual, at the gym or at work Repetitive action – think of that constant mouse or keyboard action in the office environment Overstretching of the tendon – Poor office ergonomics can overload the elbow joint and the elbow’s tendons To be more specific, the office worker presenting with elbow tendinopathy often has repetitive mouse/keyboard use, which is often accompanied by poor ergonomic factors, such as the forearm being in a prolonged pronated position (palm facing down), which places the common extensor digitorum tendon (CEDT) under stretch. Medial and Lateral Tendinopathy of the Elbow Let’s look into the difference between the actual Tennis (lateral) and Golfer’s (medial) Elbow. Tennis Elbow (Lateral Epicondylitis) Pain in the outer elbow Irritation of the wrist extensor tendons, especially the Extensor Carpi Radialis Brevis (ECRB) Familiar with typing, lifting, racquet sports, and DIY tasks Golfer’s Elbow (Medial Epicondylitis) Pain in the inner elbow Irritation of the wrist flexor tendons Related to gripping, pulling, forearm rotation, and throwing How To Recover From a Tendinopathy? Despite different pain locations, the rehab approach is almost identical, and while rest provides temporary relief, it does not fix the underlying tendon changes. The true solution? A structured, progressive exercise rehab program that restores tendon strength and resilience. In fact, as the tendinopathy itself came to be an issue due to an overload of the elbow’s tendon, to settle the pain and discomfort, we have to: Reinforce the elbow tendon and muscle so that it can perform better. Analyse what overloaded the elbow tendons – we have to understand what can be changed in the loading process, starting from: Shoulder stability (looking up in the joint chain – Mobility and Stability) The ergonomic of your workload, that is, office or heavy repetitive work (like gardening, for example, or construction). Workout program – ensure there is a progressive load in the program that is right for your capacity. The 3-Phase Exercise Program for Elbow Tendinopathy Here at Melbourne Massage and Treatment in Fitzroy North, as a clinical myotherapist, I get to see many patients presenting with Elbow Tendinopathy, and the rehab protocol and recovery that I used is detailed below. Phase 1: Pain Reduction & Tendon Activation (Week 1–3) In this initial phase, the goal is to calm symptoms without resting the tendon completely. Tendons respond best to gentle, controlled tension, better known as isometric exercises. Isometric is ideal because: Tendons have a low blood supply compared to muscles, so in order to receive the nutrients that allow the healing process to be delivered, they need long and steady engagements. A tenodon that is inflamed presents with disorganised collagen fibres, which are not running straight, and no longer form a compact line. And there is a need for a constant load to restore new fibres that can regain the tendon’s functionality. Wrist Extension Isometric (for Tennis Elbow) You will be sitting at a desk with your forearm comfortably supported by the desk, with your hand in a prone position (palm down) Slightly extend your wrist against resistance. Pain-free movement (it could be a bend or a lightweight) Hold 20 seconds, repeat 10 reps Wrist Flexion Isometric (for Golfer’s Elbow) You will be sitting at a desk with your forearm comfortably supported by the desk, with your hand in a supine position (palm up) Deliver a slight wrist flexion against resistance. Again, it has to be a pain-free movement. Hold 20 seconds, repeat 10 reps Time of hold, repetition and pain response are subjective to each individual. That’s where we would stop and focus on each individual clinical history and presentation, and adapt the elbow tendinopathy rehab program to your needs. Gentle Mobility & Dry Needling From a point of view of massage for elbow tendinopathy, there are a few techniques that work really well, especially in the early phase of recovery: Joint Mobilisation – passive movement applied to the wrist and elbow joint, to improve the range of motion of this joint and disengage the area. Dry Needling – The usage of a needle on muscle, to create a micro-inflammation and to drive more attention from the nervous system into the targeted area. Deep Tissue Massage – When dry needling is not an option, deep tissue massage can also help in creating this targeted central nervous system response. Phase 2: Strength & Tendon Remodelling (Week 3–8) This is the most critical phase, and the one that actually restores tendon health. Eccentric Wrist Extension (Tennis Elbow Gold Standard) How to do it: Extend the wrist of the affected side with your good hand, while in the affected side, you are holding a lightweight or resistance band. Slowly lower the weight with your injured side with a tempo that last 3–5 seconds Repeat 12–15 reps, 2–3 sets – this is an endurance setup. Between each set, rest for at least 30 seconds. Eccentric Wrist Flexion (Golfer’s Elbow Gold Standard) Same method, but applied in a flexion motion. Assist the initial movement of flexion Slowly bring the wrist back to the straight position with a 3-5 second tempo. Look always at somewhere between 12-15 reps, for endurance performance. […]